


What is a Nursing Report Sheet?
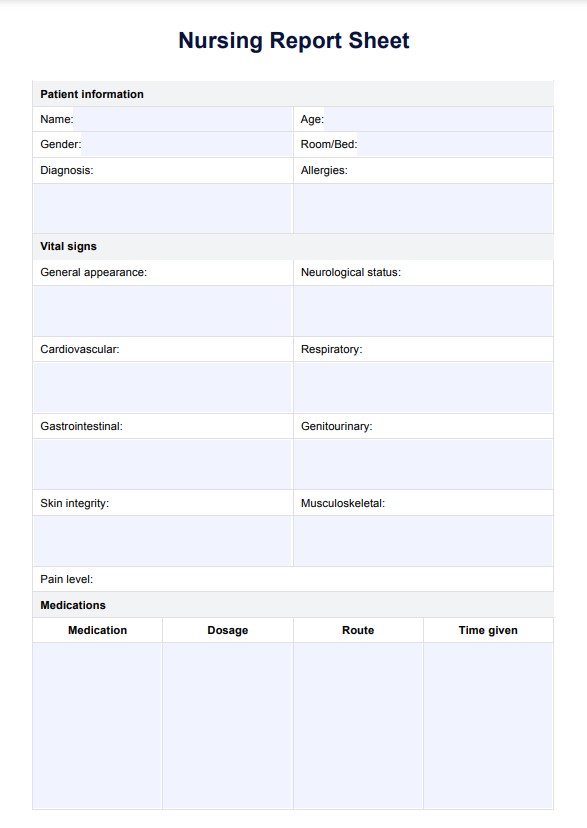
A Nursing Report Sheet, also known as a nursing brain sheet or patient report form, is a comprehensive document that healthcare professionals use to communicate all the details about a patient's condition, treatment plan, and progress during shift changes or when transferring the patient between units or facilities.
Documenting through brain sheets is vital for ensuring continuity of care and effective communication among nurses, even nursing students, and other healthcare providers. This report sheet typically contains several sections that capture the patient's medical history, current condition, and ongoing care.
These sheets are especially helpful for nursing students or new nurses, as they serve as beneficial education tools. A nurse educator can use them to help students learn how to prioritize important information, communicate effectively with other healthcare professionals, and stay organized during their clinical rotations or job experiences, even in early nursing school.









