Looking for a way to assess the severity of feelings of loneliness in your patients or clients? Read our guide to learn why examining and addressing loneliness is important for mental healthcare professionals. Then, use the UCLA Loneliness Scale to assess the loneliness your patients and clients feel.
## **Examining and addressing loneliness**
Loneliness is a profound subjective state of distress arising from a perceived deficit in social relationships, distinct from social isolation (the objective lack of contact) (Veazie et al., 2019).
Common causes often include major life transitions (e.g., relocation, job change), loss of a loved one, social exclusion or discrimination, and underlying mental health conditions like social anxiety or depression that impair social connection.
From a clinical perspective, identifying and mitigating loneliness is crucial because when these feelings are left unaddressed, they can have severe, compounding consequences. Chronic loneliness is a significant risk factor for the development and exacerbation of mental illnesses, including major depressive disorder and anxiety disorders, and is strongly linked to suicidal ideation and attempts (CDC, 2025).
Moreover, it impacts physical health, increasing the risk for cardiovascular disease, impaired immune function, cognitive decline, and premature mortality (Hawkley & Cacioppo, 2010), effectively making it a public health crisis that demands professional intervention and integrated treatment strategies.
To address loneliness, healthcare professionals must proactively screen for loneliness, using validated tools to assess both the quality and quantity of a patient's social connections.
Effective interventions move beyond simply encouraging more social contact; they focus on improving the quality of their social relations and addressing the cognitive distortions that sustain feelings of isolation (e.g., negative self-perceptions, assuming others are uninterested). Strategies may include [cognitive behavioral therapy](https://www.carepatron.com/guides/cbt-techniques) (CBT) to challenge maladaptive social thoughts, skills training to enhance social competence, and facilitating connections through structured, shared-interest groups (CDC, 2024).
## **What is the UCLA Loneliness Scale?**
The UCLA Loneliness Scale is a widely recognized tool in social psychology that measures loneliness and social isolation. Initially developed in 1978 by Russel et. al and later revised in 1980, the Revised UCLA Loneliness Scale provides a framework for assessing an individual's subjective experience of loneliness, encompassing both social and emotional loneliness. This scale has 20 items instead of just 10, evaluating how often individuals feel they lack companionship or feel isolated with informed consent, highlighting the impact of social relationships on overall well-being. Additionally, there is also a version 3 of the UCLA Loneliness Scale, created to simplify the wording of the items for greater clarity.
The Revised UCLA Loneliness Scale consists of a series of statements that participants respond to, allowing for a nuanced analysis of their social connections. The results can reveal whether individuals feel socially connected or experience a profound sense of isolation. By identifying key risk factors associated with loneliness, such as a low self-esteem or diminished social life, healthcare practitioners can better understand the emotional and psychological needs of their patients.
This UCLA scale, specifically version 3, is widely regarded as a psychometrically sound measure, demonstrating high reliability with internal consistency and strong one-year test-retest reliability (Russell, 1996). However, the scale is not without limitations: its original development largely relied on college students in the USA, raising concerns about its generalizability across all ages and cultures, though shorter versions have since been validated in older populations (Alsubheen et al., 2021).
Despite its limitations, this scale still serves as a vital tool for measuring loneliness, enabling practitioners to develop targeted interventions that enhance social relationships and improve overall mental health. Aside from that, it can also be used in research to assess the subjective experience of loneliness and social dissatisfaction across diverse populations, and increasingly in clinical and community settings for screening and evaluation.
## **How to conduct the UCLA Loneliness Scale?**
Here's a step-by-step on how to conduct the test:
### **Step 1: Help your clients familiarize themselves with the test**
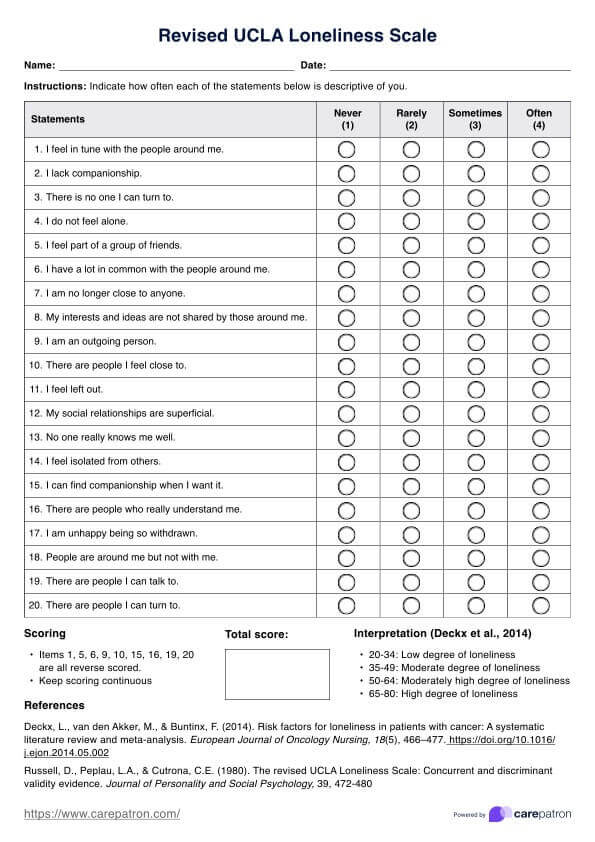
As mentioned, the UCLA Loneliness Scale-Revised consists of 20 items designed to assess loneliness, particularly focusing on emotional loneliness.
Have your clients respond to these items using a four-point Likert scale, allowing healthcare professionals to gauge the intensity of their feelings regarding loneliness.
### **Step 2: Score**
The scoring of the Revised UCLA Loneliness Scale utilizes a 4-point rating system, where participants respond to 20 questions, such as “How often do you feel left out?” and “How often do you feel part of a group of friends?” The scale ranges from 1 (never) to 4 (always).
After participants complete the questionnaire, you must reverse-score items 1, 5, 6, 9, 10, 15, 16, 19, and 20, ensuring that higher scores indicate greater feelings of loneliness. Then, calculate the respondent's score by averaging their ratings, providing a clear measure of their loneliness levels, which can inform potential interventions and support strategies.
### **Step 3: Interpret**
Higher scores, typically ranging from 65 to 80, indicate significant feelings of loneliness and social isolation. Scores in the moderately high range of 50 to 64 suggest that the individual may experience occasional feelings of loneliness, but it is not a prominent aspect of their emotional state.
Scores in the moderate range of 35 to 49 signify a moderate degree of loneliness, where individuals may feel some level of social disconnection and isolation, but it does not significantly impact their overall well-being.
Lastly, lower scores, ranging from 20 to 34, indicate a low degree of loneliness, meaning that individuals in this range feel relatively content and fulfilled with their social connections and interactions (Deckx et al., 2014).
Understanding these interpretations helps healthcare practitioners tailor their approaches, addressing both the negative impacts of loneliness on mental health and promoting strategies for building social skills and finding companionship. This nuanced interpretation aids in fostering overall well-being.
## **Next steps**
After completing the Revised UCLA Loneliness Scale, medical professionals and their patients should engage in a collaborative discussion about the results.
### **Targeted interventions**
For patients with high loneliness scores, practitioners may recommend targeted interventions, such as counseling, [social skills](https://www.carepatron.com/templates/social-skills-worksheet/) training, or support groups, to enhance social connections. Patients should also be encouraged to identify and participate in activities that foster community engagement.
### **Reinforcing healthy social habits**
For those with lower scores, reinforcing healthy social habits and promoting continued involvement in social activities can be beneficial. Regular follow-up assessments using the UCLA Loneliness Scale can help monitor progress and adapt strategies as needed, ensuring ongoing support for emotional well-being.
## **References**
Alsubheen, S. A., Oliveira, A., Habash, R., Goldstein, R., & Brooks, D. (2021). Systematic review of psychometric properties and cross-cultural adaptation of the University of California and Los Angeles loneliness scale in adults. Current Psychology, 42(14), 11819–11833. https://doi.org/10.1007/s12144-021-02494-w
CDC. (2024, May 22). Promising Approaches to Promote Social Connection. Social Connection. https://www.cdc.gov/social-connectedness/data-research/promising-approaches/index.html
CDC. (2025, February 3). Health Effects of Social Isolation and Loneliness. Social Connection. https://www.cdc.gov/social-connectedness/risk-factors/index.html
Deckx, L., van den Akker, M., & Buntinx, F. (2014). Risk factors for loneliness in patients with cancer: A systematic literature review and meta-analysis. European Journal of Oncology Nursing, 18(5), 466–477. https://doi.org/10.1016/j.ejon.2014.05.002
Hawkley, L. C., & Cacioppo, J. T. (2010). Loneliness Matters: A Theoretical and Empirical Review of Consequences and Mechanisms. Annals of Behavioral Medicine, 40(2), 218–227. https://doi.org/10.1007/s12160-010-9210-8
Russell, D., Peplau, L.A., & Cutrona, C.E. (1980). The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. Journal of Personality and Social Psychology, 39, 472-480
Russell, D. W. (1996). UCLA Loneliness Scale (Version 3): Reliability, Validity, and Factor Structure. Journal of Personality Assessment, 66(1), 20–40. https://doi.org/10.1207/s15327752jpa6601_2
Veazie, S., Gilbert, J., Winchell, K., Paynter, R., & Guise, J.-M. (2019, February). Social Isolation and Loneliness Definitions and Measures. Nih.gov; Agency for Healthcare Research and Quality (US). https://www.ncbi.nlm.nih.gov/books/NBK537897/#:~:text=Social%20isolation%3A%20An%20objective%20lack,6