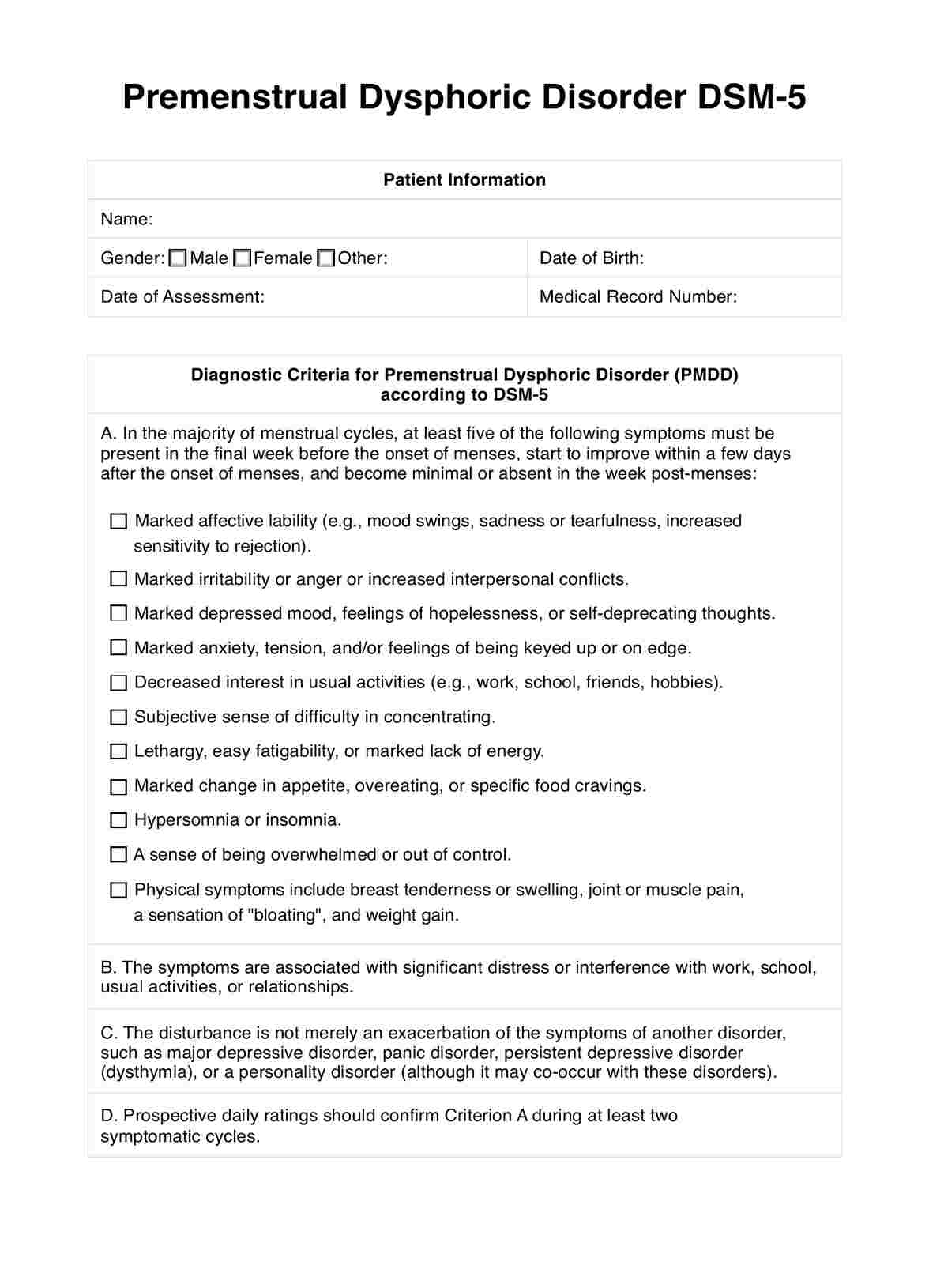
What is PMDD according to the DSM-5?
Premenstrual Dysphoric Disorder (PMDD) is a condition classified in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) under depressive disorders. It is characterized by severe mood symptoms, emotional disturbances, and physical symptoms occurring during the late luteal phase of most menstrual cycles. PMDD symptoms markedly interfere with daily functioning and result in clinically significant distress. These symptoms may include marked irritability, mood swings, depressed mood, feelings of sadness, anger, anxiety, marked affective lability, and decreased interest in usual activities.
Physical symptoms commonly associated with PMDD include joint or muscle pain, breast tenderness, weight gain, food cravings, major depression, and other somatic symptoms. These symptoms typically appear following ovulation and improve with the onset of menses.
PMDD diagnosis requires the presence of specific depressive symptoms during most menstrual cycles and their resolution shortly after menstruation begins. Risk factors for PMDD include hormonal fluctuations, reproductive hormones, and underlying mood disorders such as major depressive disorder or persistent depressive disorder.
Treatment for PMDD may involve psychotherapy, lifestyle changes, and medication, including selective serotonin reuptake inhibitors (SSRIs) to alleviate symptoms. It's crucial to differentiate PMDD from other mood disorders, premenstrual syndrome (PMS), and medical conditions to provide appropriate management and support to individuals affected by this condition.









