Everyone has a story to tell, and here we share and celebrate those who chose care as their life's work.
These are their words, their work and we're grateful to share them.
Elizabeth and Dennis handed their billing to Carepatron and grew My Therapeutic Concepts from five clients to seventy in two months, without losing their evenings.
After a pregnant mother gives birth, it's normal for them to go through a stage called postpartum depression or postnatal depression. The degree to which they'll be affected by this will vary from person to person, but even the mildest level of this kind of depression shouldn't be taken lightly because it could always just warp into major depression down the line.
If you specialize in handling pregnant women for your healthcare practice or are part of a preventive services task force, and you're looking for a tool beyond basic ones like the Patient Health Questionnaire to help you assess a mother going through postnatal depression, continue reading our guide to learn more about the nifty Edinburgh Postnatal Depression Scale (EPDS). Then, download our template so you can examine the severity of postnatal depression in your female patients!
## **What is postpartum depression?**
Postpartum depression, also known as postnatal depression, is a type of clinical depression that can develop in women after giving birth. Unlike the "baby blues," which is a mild and temporary mood disturbance, postpartum depression is a more severe and longer-lasting form of depression that can significantly impair a woman's ability to function and care for herself and her baby (Banti et al., 2011).
Symptoms of depression with an onset during or after pregnancy can include persistent feelings of sadness, loss of interest or pleasure in activities, excessive guilt or worthlessness, fatigue, changes in appetite, difficulty sleeping, and, in severe cases, suicidal thoughts (American Psychiatric Association, 2013).
It is important to note that depression among pregnant and postpartum women is not a character flaw or a sign of weakness. Postpartum depression, along with perinatal depression, is a treatable medical condition that requires professional help and support.
Postpartum depression comes with symptoms characteristic of non-postpartum depression. Severe symptoms include losing interest in their child and what their child likes doing, as well as severe mood swings. More severe symptoms include self-harm or harming the baby, and withdrawal from loved ones, especially the child, because of guilt and shame.
If postpartum depression is left alone, it could develop into severe depression (major depressive disorder). It can also prevent the mother from eating well, which could also lead to a lack of energy to care for their child, and if they don't have the energy or motivation to care for their child, the child runs the risk of developing behavioral problems and having developmental delays. Extreme cases involve the mother having self-harming behaviors and/or the tendency to hurt their baby (Postpartum Depression Causes, Symptoms, and Treatments, n.d.).
## **What is the Edinburgh Postnatal Depression Scale (EPDS)?**
The Edinburgh Depression Scale is a widely used screening tool for identifying possible depression in the general population. It is a self-report questionnaire that assesses various symptoms associated with depression.
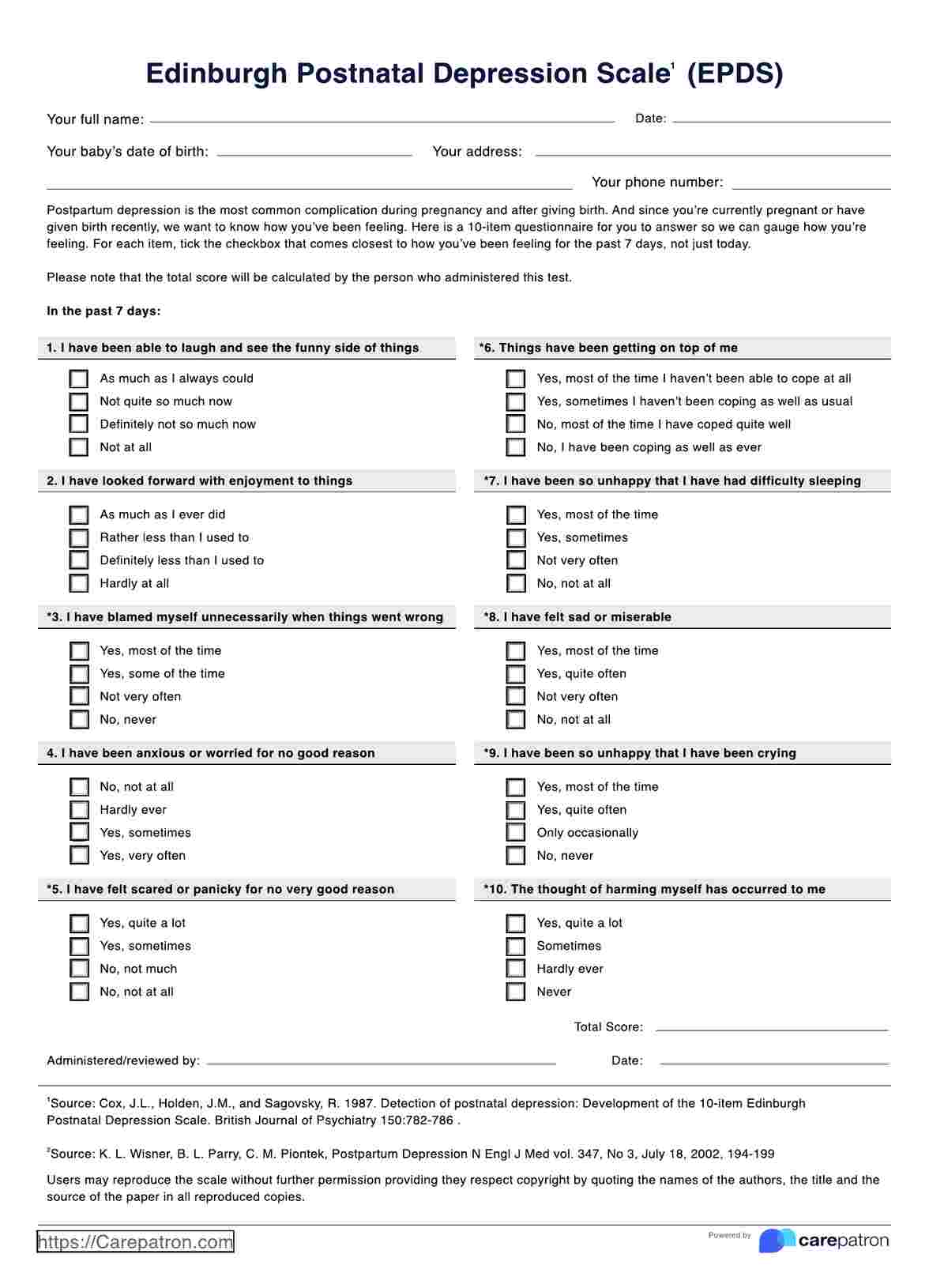
The EPDS is a specific version of the Edinburgh Depression Scale that has been adapted and validated for screening postpartum depression in new mothers. It is a 10-item self-report questionnaire that assesses symptoms of depression experienced within the past seven days (Banti et al., 2011).
The EPDS was developed to identify women who may have postnatal depression, which is a significant public health concern affecting many women during the postpartum period. Unlike the general Edinburgh Depression Scale, the EPDS focuses on symptoms that are particularly relevant to the postpartum period and difficulty coping with everyday tasks related to caring for a newborn.
Women with pre-existing mental health conditions, such as anxiety disorders, bipolar disorder, or other personality disorders, may be at higher risk for developing postpartum depression. In these cases, regular screening with the EPDS can help monitor their mental health and provide early intervention if necessary.
Certain factors, such as a history of depression, lack of social support, or stressful life events, can increase a woman's risk of developing postpartum depression. Healthcare providers may choose to screen more frequently or at earlier time points for women with these risk factors.
### **Considerations before using the tool**
The EPDS has been evaluated for its predictive value in identifying postpartum depression. It can be inaccurate and would better serve as an initial assessment rather than the one guiding treatment decisions for postnatal depression moving forward (Meijer et al., 2014).
It also has some limitations worth considering, such as having ambiguous items, the exclusion of certain kinds of distress, scoring difficulties, and frequent use of incorrect cut-off scores (Matthey & Agostini, 2017).
Given all this, it doesn't mean you shouldn't use this tool. You can still use it, but make sure to use other tools that detect major depression.
## **How to use the Edinburgh Postnatal Depression Scale (EPDS)**
Using the Edinburgh Postnatal Depression Scale as a screening tool for postpartum depression can be done with the following steps:
### **Step 1: Administration**
The EPDS is a 10-item self-report questionnaire that should be administered to the mother for her completion. Ensuring that the mother understands the instructions and feels comfortable answering the questions honestly is important. Of course, you can opt to conduct this assessment as a structured clinical interview where you ask the items as questions and they rate themselves based on the choices.
### **Step 2: Scoring and interpretation**
Each item in the EPDS is scored on a scale of 0 to 3, with a maximum total score of 30. Higher scores indicate a greater likelihood of depression. The EPDS scores' positive predictive values help determine the likelihood of postpartum depression, enhancing the accuracy of the screening process.
### **Step 3: Clinical judgment**
It is crucial to understand that the EPDS is a screening tool and should not override clinical judgment on its own. The score should be interpreted in conjunction with careful clinical assessment, considering factors such as the presence of other mental health conditions, the severity of symptoms, and the overall clinical picture.
### **Step 4: Follow-up and support**
For women who screen positive for EPDS or who express concerns about their mental health, it is important to provide appropriate follow-up care, which may include referral to a mental health professional, support groups, or other resources.
## **Scoring and interpretation**
Each item has its own unique answer set. Mothers must pick one answer from each set based on their feelings for the last seven days before answering the scale. Each item can get a possible score of 0 to 3, and it will depend on their answer choice.
Items 1, 2, and 4 are scored 0 to 3. The answers are arranged as such:
- The first choice is worth 0 points
- The second choice is worth 1 point
- The third choice is worth 2 points
- The last choice is worth 3 points
Items 3 and 5 to 10 are scored 3 to 0, meaning they are reverse-scored. The first choice is worth 3 points, the second is worth 2 points, the third is worth 1 point, and the last is equal to 0. Add up to get the total EPDS score. The possible maximum score that each patient can get is 30.
The Edinburgh Postnatal Depression Scale doesn't have a single optimal cut-off value. There are only two things you need to consider when interpreting the scores on the scale:
- A score of 10 to 30 means that the mother possibly has depression symptomatology, so you will need to conduct a careful clinical assessment and use clinical judgment before diagnosis (Navaratne et al., 2016).
- The last item deals with self-harm. If they tick the first or second answer choice, that's a cause for concern. Even if the total score from Items 1 to 9 is 0, but they picked the first or second answer choice for Item 10, you must find a way to address their thoughts of self-harm.
This downloadable EPDS Scoring Handout can be a helpful tool in this stage of the assessment process.
Also, again, the scoring for this is considered to be vague by some researchers, and you might, too! While it may identify depression, it doesn't have any designations like "mild depression" or "moderate depression." Further evaluation is needed to get consistent results so you can make a formal diagnosis and a better informed view of what needs to be done for the patient.
## **Other depression-related assessments you can use**
If you're looking for more tools to help you assess depression in mothers going through postnatal depression, here are some tools you can consider using for your clinical practice:
- **Beck Depression Inventory**: This tool assesses symptoms of major depressive disorder, and it zooms into feelings about the future, loss of motivation, and expectations, which you may want to examine, considering these are things that mothers with postnatal depression will likely grapple with.
- **Zung Self-Rating Depression Scale**: This is another scale that is self-rated and pinpoints specific feelings or experiences that people have, like having crying spells, trouble sleeping, if they eat well or not, being irritable, etc.
- **Hamilton Depression Scale**: This scale is used by you, andyou rate the patient based on your observations while talking to them. You basically rate them for their mood, feelings of guilt, their feelings towards their work and interests, suicidal ideation/action, etc.
While these tools don't focus on postnatal depression, they can at least be used to cover as much ground as possible when it comes to assessing someone for depression. Our templates for these are easy to use, and you only need to tick the specific ratings/answers accordingly based on each scales specifications.
## **References**
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Pearson.
Banti, S., Mauri, M., Oppo, A., Borri, C., Rambelli, C., Ramacciotti, D., Montagnani, M. S., Camilleri, V., Cortopassi, S., Rucci, P., & Cassano, G. B. (2011). From the third month of pregnancy to 1 year postpartum. Prevalence, incidence, recurrence, and new onset of depression. Results from the perinatal depression-research & screening unit study. Comprehensive Psychiatry, 52(4), 343–351. https://doi.org/10.1016/j.comppsych.2010.08.003
Matthey, S., & Agostini, F. (2017). Using the Edinburgh Postnatal Depression Scale for women and men—some cautionary thoughts. Archives of Women S Mental Health, 20(2), 345–354. https://doi.org/10.1007/s00737-016-0710-9
Meijer, J., Beijers, C., Van Pampus, M., Verbeek, T., Stolk, R., Milgrom, J., Bockting, C., & Burger, H. (2014). Predictive accuracy of Edinburgh Postnatal Depression Scale assessment during pregnancy for the risk of developing postpartum depressive symptoms: a prospective cohort study. BJOG an International Journal of Obstetrics & Gynaecology, 121(13), 1604–1610. https://doi.org/10.1111/1471-0528.12759
Navaratne, P., Foo, X. Y., & Kumar, S. (2016). Impact of a high Edinburgh Postnatal Depression Scale score on obstetric and perinatal outcomes. Scientific Reports, 6, 33544. https://doi.org/10.1038/srep33544
Postpartum depression causes, symptoms, and treatments. (n.d.). UPMC | Life Changing Medicine. https://www.upmc.com/services/womens-health/conditions/postpartum-depression#:~:text=Complications%20of%20Postpartum%20depression&text=They%20may%20not%20eat%20well,infants%20whose%20parents%20have%20PPD.
Commonly asked questions
The Edinburgh Postnatal Depression Scale (EPDS) is a 10-item self-report questionnaire used to screen for symptoms of postnatal depression in new mothers. It helps healthcare professionals identify emotional and psychological distress that may develop after childbirth. Each item is scored on a scale of 0 to 3, reflecting how the mother has felt during the previous seven days.
A normal EPDS score typically ranges from 0 to 9, suggesting no or minimal signs of depression. Scores between 10 and 12 indicate possible mild depression and warrant further observation. A score of 13 or higher suggests a high likelihood of postpartum depression and should prompt a comprehensive clinical assessment.
The EPDS measures the intensity of depressive symptoms such as sadness, anxiety, guilt, and sleep or appetite changes in postpartum individuals. It focuses on emotional and cognitive symptoms rather than physical ones, making it suitable for distinguishing depression from normal postnatal fatigue. Its main goal is early detection to enable timely intervention and support for maternal mental health.