


What is an MDS Assessment Cheat Sheet?
A minimum data set (MDS) assessment is a standardized evaluation used in elderly healthcare to record the functional ability and health of a nursing home resident. It records current health concerns and facilitates appropriate, individualized care. Federal law requires all residents of Medicare and Medicaid-certified facilities to undergo periodic MDS assessments.
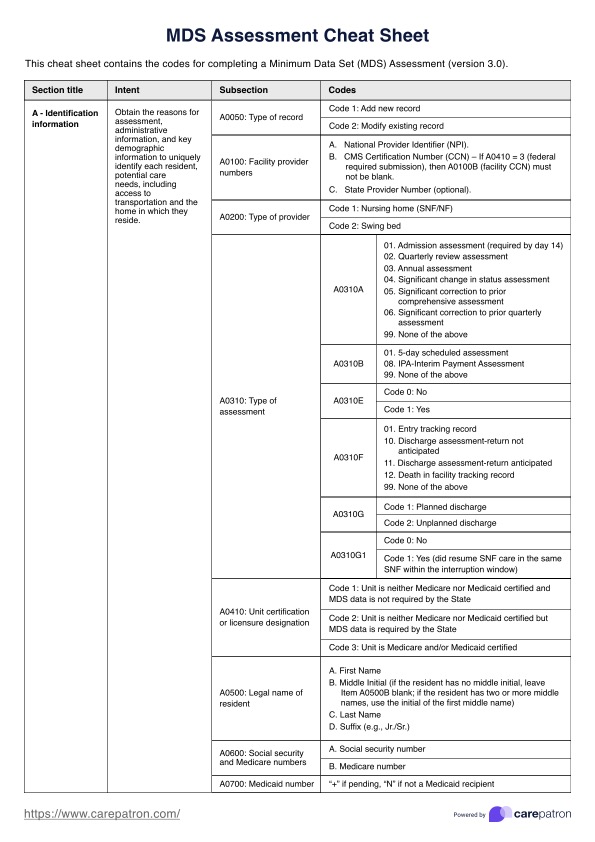
An MDS Assessment Cheat Sheet serves as a quick reference tool to aid nursing home staff in accurately completing the assessment. This resource guides staff through the different sections of the evaluation, such as daily living activities, medication usage, oral hygiene, and specific diagnoses, focusing on the resident's condition within the prior seven days.
This comprehensive assessment plays a pivotal role in measuring the health status of residents and initiating comprehensive care plans. Regulatory standards require these assessments to be conducted at specific intervals, including when a resident first arrives, is discharged, or displays a significant change in condition.
A cheat sheet is a simple way to ensure this meticulous process is completed accurately, ensuring a reliable evaluation of the resident's health status. By conducting MDS assessments with precision, nursing home staff contribute to creating a comprehensive and personalized care record, aligning with regulatory standards and fostering optimal resident well-being.









