


What are activities of daily living (ADLs)?
Activities of daily living (ADLs) are routine aspects of daily functioning essential for self-care and independence. Specific ADLs include basic self-care tasks like eating, bathing, dressing, toileting, bed mobility, transferring (moving from a bed to a chair), maintaining personal hygiene, and continence. They are foundational skills typically learned in early childhood.
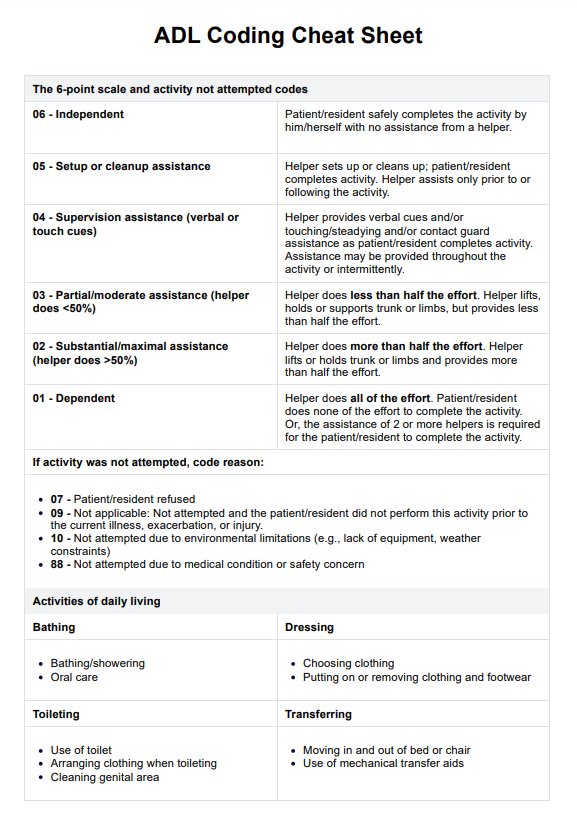
ADLs are coded in healthcare settings to assess patients' functional status on a spectrum of self-care ability, from complete independence to total dependence on caregivers. This aids in determining the level of assistance a patient requires with daily activities and their specific care needs.
ADL coding involves observing and assessing an individual's ability to perform these activities. Healthcare providers use a standardized coding system to document the extent to which each ADL can be done independently, determining the overall ADL score. Accurate ADL documentation is critical for creating effective care plans, ensuring appropriate staffing and resources, and facilitating communication among the healthcare team and family members.
Inaccurate or incomplete ADL coding can lead to inadequate care plans, affecting a patient's recovery and overall well-being. It can also impact billing and reimbursement processes in healthcare facilities. Accurate ADL documentation is a cornerstone of quality healthcare and essential to high-quality care and efficient healthcare operations.









