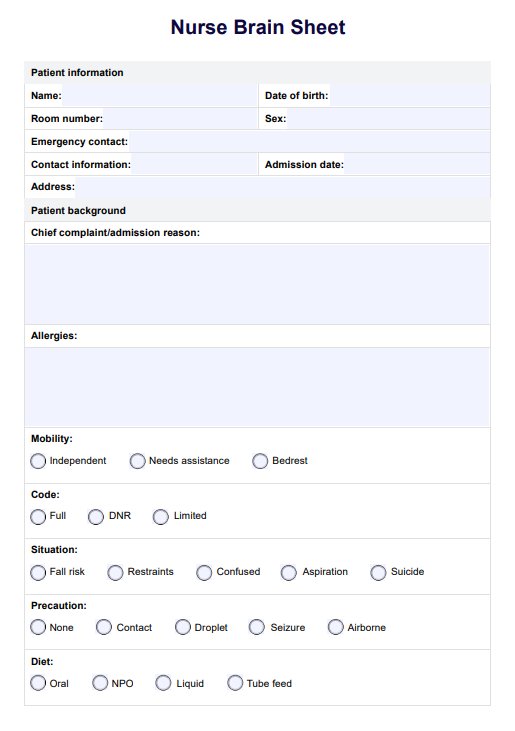
When should you use this Nurse Brain Sheet?
Our Nurse Brain Sheet Template is a versatile resource designed for various healthcare practitioners. It provides a structured approach to patient care in various clinical scenarios.
Regular patient shifts
Nurses handling regular shifts benefit from the template's comprehensive layout, which ensures a systematic tracking of vital signs, medications, and assessments. Its user-friendly format facilitates a quick overview of each patient's status, allowing for efficient documentation or anything necessary to write things down, decision-making, and care planning. The template is a reliable communication tool during shift changes or patient handovers. It enables a seamless transition of care between healthcare practitioners by consolidating essential patient data, ensuring continuity, and minimizing the risk of information gaps.
Emergencies
In high-stress emergencies, the Nurse Brain Sheet Template becomes invaluable. Its organized structure aids in quickly grasping critical patient information, enhancing rapid response and timely interventions during crises.
Multidisciplinary collaboration
The template fosters effective communication among diverse practitioners in collaborative healthcare settings, such as intensive care units or surgical teams. Physicians, nurses, and allied health professionals can easily share and comprehend essential surgical or ICU patient information.
Long-term care planning
The template aids in developing and monitoring long-term care plans for patients requiring extended care or those managing chronic conditions. Its adaptability accommodates evolving patient needs, providing a holistic view of their healthcare journey.
New admissions
This template guides practitioners in swiftly recording pertinent information when receiving new patients, whether in an acute care setting or clinic. This ensures a comprehensive understanding of the patient's history and immediate needs, facilitating a smooth integration into the care environment.
Teaching and training
The template is an excellent teaching aid for educators and trainers for a nursing student or new healthcare practitioner. It instills the importance of systematic data collection and organization in delivering high-quality patient care and education.
The Nurse Brain Sheet Template is indispensable in numerous healthcare scenarios, promoting efficiency, collaboration, and optimal patient outcomes across diverse clinical settings. Its adaptability makes it a go-to tool for healthcare practitioners seeking to enhance their approach to patient care.
Explore our Care Plan Template for added support in improving your practice and client results.