Looking for a tool that can help you assess a patient's functional independence? Read our guide to learn more about functional independence, then use the Modified Barthel Index to measure your patient's functional independence to determine what they can do by themselves or with assistance, and what they can't do, so you can determine how to improve their functional independence.
## **The importance of functional independence**
Functional independence is a crucial aspect of our lives because it reflects our ability to perform certain tasks independently, particularly activities of daily living (ADLs). These activities are the most basic things we do each day, from feeding ourselves, bathing, getting dressed, and simply moving ourselves around. Being unable to do any of these by ourselves can significantly reduce our overall quality of life.
Examples of problems that can negatively impact functional independence include injuries due to falls or accidents, disabilities because of musculoskeletal disorders, neurological problems, cancer, etc. Examples of people who have to deal with weakened functional independence (or have become functionally dependent) include stroke patients/those with chronic stroke, oncology patients, those with Parkinson's disease, those with broken limbs, etc.
Loss of functional independence can lead to all sorts of mental health issues, too, especially in the elderly who once enjoyed being spry and able to do things like exercising and going on adventures. They could become depressed because they can no longer do what they were able to do without assistance, or are unable to do them at all. They might isolate themselves. They might even be so dejected that they desire (possibly unconsciously) to be functionally dependent on others (Yesavage & Sheikh, 1986).
Whether you work in physical therapy or occupational therapy, it's your job to find ways to rehabilitate your patients and hopefully restore their functional independence (this might not be possible for some, like victims of severe burns, those who are already bedridden, etc.). To help you determine what you can do, it would be best to use assessments that examine a patient's functional independence or lack of it, like the Modified Barthel Index.
## **What is a Modified Barthel Index?**
Before discussing the Modified Barthel Index, let's briefly discuss what the Barthel Index is.
The Barthel Index is a well-regarded performance evaluation tool in physical and rehabilitation medicine, particularly for assessing functional independence in individuals, including stroke patients admitted to hospitals or at home (Sulter et al., 1999). This index has two modified versions, developed in the 1960s by Dr. Florence Mahoney and Dorothea W. Barthel.
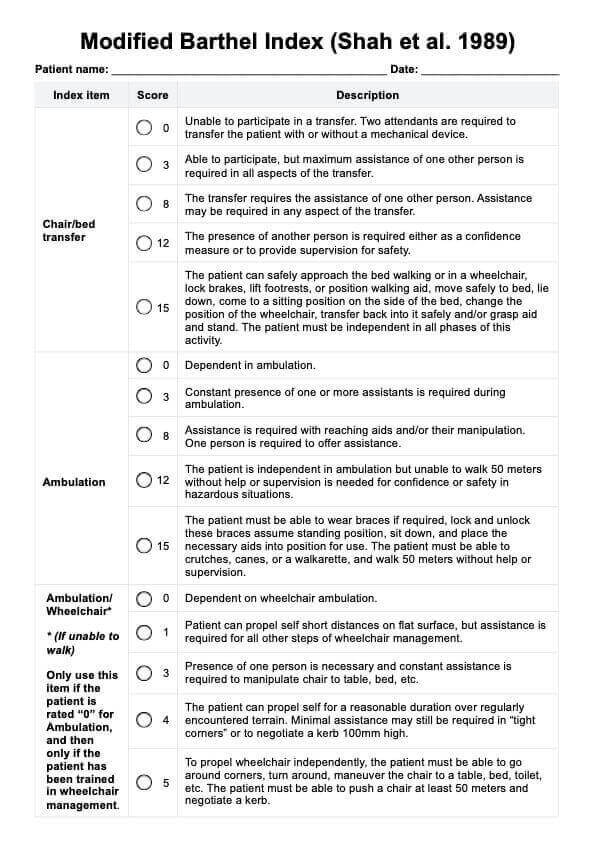
In 1988, Collin et al. revised the scoring system of the index to utilize 1-point increments, resulting in a total score that ranges from 0 to 20. This adjustment was made to address the “disproportionate impression of accuracy” (Collin et al., 1988). Subsequently, in 1989, Shah et al. further refined the outcome measure to enhance its sensitivity and reliability in assessing stroke rehabilitation outcomes, including inpatient rehabilitation. The Shah Modified Barthel Index retains the original scoring range of 0-100, but it introduced varying point increments to improve both reliability and sensitivity in detecting changes.
### **Why you should use the Modified Barthel Index**
Carepatron has created a template based on the Shah et al. version. This Modified Barthel Index (MBI) is a comprehensive instrument for measuring an individual's capacity to perform essential activities of daily living (ADLs). The assessment is especially valuable for evaluating the functional status of patients recovering from strokes or other brain injuries.
The Modified Barthel Index by Shah and colleagues, along with the Functional Independence Measure, is one of the most widely used tools for assessing functional independence in individuals with disabilities. While the original Barthel Index effectively captures significant changes in activities of daily living, it may overlook smaller yet meaningful incremental improvements.
For patients demonstrating substantial progress, both indices show similar responsiveness. However, the Modified Barthel Index (Shah version) is specifically tailored to identify more subtle changes in a patient's ADL performance, making it particularly advantageous in rehabilitation settings where gradual improvements are common (Wang et al., 2022), so using this version can improve functional outcomes.
Besides (ischemic) stroke patients/stroke survivors, you can also use this to assess elderly patients, those with orthopedic diseases and pathologies, those with musculoskeletal disorders, and those with severe disabilities caused by injuries, burns, and illnesses.
### **Is it reliable?**
To put things into perspective, the regular Barthel Index is a highly-regarded tool. Whether you're assessing patients for the first time or if you're monitoring patients during early rehabilitation, the Barthel Index is helpful when it comes to examining patients.
The Barthel Index has excellent inter-rater reliability when it comes to early inpatient rehabilitation (Rollnik, 2011). It also has adequate to excellent inter-rater reliability when it comes to assessing geriatric rehabilitation for patients with stroke and Parkinson's disease (Castiglia, 2017).
So, yes. It is reliable. This modified version can be trusted and gives you more ground to work with because it has more rating options that zoom in on the smaller things when it comes to patients.
## **How to use our Modified Barthel Index template**
To maximize this tool in your clinical practice, follow these steps:
### **Step 1: Download the free MBI template**
To use the Modified Barthel Index (Shah version) template in the Carepatron app, just click the "Use Template" button. If you prefer, you can also click the "Download" button to get a PDF copy.
### **Step 2: Familiarize yourself with the index**
Before assessing your patient, it is essential to understand the different components of the Modified Barthel Index and how they are scored. Familiarize yourself with the scale and scoring methods to ensure accurate and consistent evaluations.
It pretty much works like the regular Barthel Index. It is divided into different categories, including bowel control, bladder control, stair climbing, ambulation, etc. You just need to tick the rating appropriate for your patient based on your observations. Scoring choices and rating descriptions are all different for each category, so please rate according to the descriptions.
### **Step 3: Conduct a comprehensive assessment**
When conducting an MBI assessment, it is crucial to observe your patient's performance in each activity instead of relying solely on their self-report. This approach can provide more reliable results and better reflect a patient's functional status because you'll witness firsthand if the patient requires assistance or not.
### **Step 4: Document any changes in performance**
As mentioned earlier, the Modified Barthel Index (Shah version) is particularly useful for detecting subtle improvements in ADL performance. Therefore, accurately documenting any changes observed during subsequent assessments is important. These changes can also help inform treatment plans and track progress over time.
### **Step 5: Use the MBI in conjunction with other assessment tools**
While the Modified Barthel Index is a valuable tool, it should not be used as the sole measure to evaluate a patient's functional status. Use it in conjunction with other clinical assessments and observations to gain a comprehensive understanding of a patient's overall functioning.
### **Step 6: Review and update regularly**
As a patient's condition can change over time, it is essential to review and update their MBI score regularly. This ensures that their treatment plan and care needs are continuously reassessed and adjusted accordingly.
## **Scoring and interpretation**
The Modified Barthel Index developed by Shah et al. (1989) includes specific items that evaluate various forms of assistance needed by individuals. These items cover assistance required for ambulation, feeding, bathing, personal hygiene, and dressing. Additionally, it assesses the presence or absence of fecal and urinary incontinence and the support required for transfers, walking, and climbing stairs.
The sum scores in the MBI are calculated by summing the individual item scores, with a maximum possible score of 100, indicating complete functional independence. The interpretation of the total final score is typically based on the following guidelines:
- **91–99**: Slight dependency
- **61–90**: Moderate dependency
- **21–60**: Severe dependency
- **0–20**: Total dependency
## **How is this different from the regular index?**
The original index was designed as a three-item ordinal rating scale, with certain items utilizing a four-item scale. It includes ten items evaluated based on an individual's ability to perform a task or activity independently, with assistance, or with complete dependence.
According to Sinoff and Ore (1997), the scoring on the Barthel Index (BI) can be interpreted as follows:
- A score of 80-100 indicates independence
- A score of 60-79 suggests minimal assistance is needed with activities of daily living
- A score of 40-59 reflects partial dependence
- A score of 20-39 signifies high dependence
This version by Shah et al. (1989) also has 10 items (with two items combined for ambulation) and varying rating options based on the item assessed. For example, for feeding, instead of using the simple scoring system, this version's rating options are as follows:
- 0: Dependent in all aspects and needs to be fed, nasogastric needs to be administered.
- 2: Can manipulate an eating device, usually a spoon, but someone must provide active assistance during the meal.
- 5: Able to feed self with supervision. Assistance is required with associated tasks such as putting milk/sugar into tea, salt, pepper, spreading butter, turning a plate or other “set up” activities.
- 8: Independence in feeding with prepared tray, except may need meat cut, milk carton opened or jar lid etc. The presence of another person is not required.
- 10: The patient can feed self from a tray or table when someone puts the food within reach. The patient must put on an assistive device if needed, cut food, and if desired use salt and pepper, spread butter, etc.
## **Similar tools you can use**
- **Berg Balance Scale**: The [Berg Balance Scale](https://www.carepatron.com/templates/berg-balance-scale) is meant to be used on elderly patients. The purpose of this scale is to assess their balancing capabilities and risk of falling. It has 14 items. You rate your patient from 0 to 4 based on balancing prompts. Balance is important when it comes to functional independence, so this is another tool you might want to use alongside patients, assuming it has been confirmed that their balancing capabilities have been impacted.
- **Modified Rankin Scale**: The [Modified Rankin Scale](https://www.carepatron.com/templates/modified-rankin-scale-mrs) is a tool that's used to assess patients who've had a stroke. You only have to rate the patient between 0 to 6 based on your observations of them. This rating is an overall impression of the patient's capabilities post-stroke, with higher scores indicating severe disability (and possibly death).
- **Functional Independence Measure**: The [Functional Independence Measure](https://www.carepatron.com/templates/functional-independence-measure) is often used alongside the regular Barthel Index. It was also subject to validation studies alongside it. It's an 18-item assessment tool that evaluates a patient's level of functional independence in self-care, mobility, communication, and social cognition. You will rate them between 1 to 7 during the time they're admitted into your facility, time of discharge, and during follow-ups after discharge.
## **References**
Castiglia, S. (2017b). The culturally adapted Italian version of the Barthel Index (IcaBI): assessment of structural validity, inter-rater reliability and responsiveness to clinically relevant improvements in patients admitted to inpatient rehabilitation centers. Functional Neurology, 32(4), 221. https://doi.org/10.11138/fneur/2017.32.4.221
Collin, C., Wade, D. T., Davies, S., & Horne, V. (1988). The Barthel ADL index: A reliability study. International Disability Studies, 10(2), 61–63. https://doi.org/10.3109/09638288809164103
Physiopedia. (2019). Barthel Index. https://www.physio-pedia.com/Barthel_Index
Rollnik, J. D. (2011). The Early Rehabilitation Barthel Index (ERBI). Die Rehabilitation, 50(06), 408–411. https://doi.org/10.1055/s-0031-1273728
Shah, S., Vanclay, F., & Cooper, B. (1989). Improving the sensitivity of the barthel index for stroke rehabilitation. Journal of Clinical Epidemiology, 42(8), 703–709. https://doi.org/10.1016/0895-4356(89)90065-6
Sinoff, G., & Ore, L. (1997). The barthel activities of daily living index: Self-Reporting versus actual performance in the old-old (≥ 75 years). Journal of the American Geriatrics Society, 45(7), 832–836. https://doi.org/10.1111/j.1532-5415.1997.tb01510.x
Sulter, G., Steen, C., & Jacques De Keyser. (1999). Use of the Barthel index and modified Rankin scale in acute stroke trials. Stroke, 30(8), 1538–1541. https://doi.org/10.1161/01.str.30.8.1538
Wang, Y.-C., Chang, P.-F., Chen, Y.-M., Lee, Y.-C., Huang, S.-L., Chen, M.-H., & Hsieh, C.-L. (2022). Comparison of responsiveness of the barthel index and modified barthel index in patients with stroke. Disability and Rehabilitation, 45(6), 1–6. https://doi.org/10.1080/09638288.2022.2055166
Yesavage, J. A., & Sheikh, J. I. (1986). Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clinical Gerontologist, 5(1-2), 165–173. https://doi.org/10.1300/j018v05n01_09