Everyone has a story to tell, and here we share and celebrate those who chose care as their life's work.
These are their words, their work and we're grateful to share them.
Elizabeth and Dennis handed their billing to Carepatron and grew My Therapeutic Concepts from five clients to seventy in two months, without losing their evenings.
Activities of daily living are an essential part of every person's life because they are pretty much what we do to get around. These include being able to wash ourselves and practice good hygiene, the capability to dress ourselves, feeding ourselves during meal times, being able to go to the toilet for number one and two, having the capability to transfer ourselves from the bed to a seat or what have you, and simply moving ourselves anywhere.
Being unable to do any one of these due to an injury or disability will negatively impact our functional independence and our overall quality of life. If you're handling patients who struggle with performing activities of daily living independently, consider adding the Barthel Index to your roster of assessment tools. This will enable you to evaluate their ability to perform ADLs, particularly if falls, neurological problems, or other factors have negatively impacted them.
## **What is the Barthel Index?**
The Barthel Index (or simply BI for short) is a widely used functional evaluation measure that assesses a person's ability to perform activities of daily living (ADLs). Developed by Mahoney and Barthel (1965), it was initially created for healthcare professionals to measure functional and physical disability in stroke survivors. However, its usefulness has extended to a broader range of conditions, including:
- Musculoskeletal disorders
- Neuromuscular or musculoskeletal disorder
- Brain injury
- Mental disorders
- Multiple sclerosis
- Hospital discharge planning
- Nursing home care
- Stroke and post-stroke care
The BI, a widely used functional outcomes measure, is a ranked scale with ten items, each focusing on a specific ADL. These include:
- Feeding
- Bathing
- Grooming
- Dressing
- Bowel control
- Bladder control
- Toilet use
- Transfer (moving between sitting and standing)
- Mobility (on level surfaces)
- Stair climbing
The core concept behind the Barthel Index is functional independence. This refers to a person's ability to manage daily tasks without assistance. The Barthel Index measures a patient's progress in functional recovery, which is regaining independence after an illness or injury.
It's best used when assessing stroke patients or those with other neurological problems like Parkinson's disease, for patient monitoring (especially when assessing them for gradual functional decline), making plans for patients before they're discharged, so the necessary assistance and interventions can be accounted for, and determining what rehabilitation would look like for them.
### **Just how reliable is the Barthel Index?**
As with any measure, professionals often test them on control groups to determine their psychometric characteristics. In particular, it is to find out how reliable and consistent it is (the criterion validity). For example, the group of Liu et al. (2004) used it to assess patients who have had single-incident brain injuries (e.g., vascular brain injury, traumatic brain injury, other forms of brain injury). Through their reliability study, they have determined that this measure has adequate predictive validity, in which the admission score of the index was predictive of the discharge score, meaning the low admission scores are indicative of greater changes in the patient's rehabilitation.
For Rollnik (2011), the Barthel Index has excellent inter-rater reliability when it comes to early inpatient rehabilitation for those who have had their functional independence and ADLs impacted by neurological problems, although he used the [Modified Barthel Index](https://www.carepatron.com/templates/modified-barthel-index/) for this.
Castiglia's findings suggest that this measure has adequate to excellent inter-rater reliability when it comes to assessing geriatric rehabilitation for patients with stroke and Parkinson's disease, though he used the Italian version of the index (Castiglia, 2017). They also determined that this tool has excellent internal consistency after assessing the ADL-related capabilities of those undergoing rehabilitation for internal diseases (e.g., metabolic, cardiorespiratory), neurological problems (e.g., stroke, Parkinson's disease), and orthopedic pathologies (e.g., vertebral problems, post-surgery).
Regardless of the version and language, it's safe to say that the Barthel Index generally exhibits good psychometric properties. It's no wonder that it's a widely used measure when assessing patients for their functional independence almost everywhere.
Whether you're assessing community-dwelling older adults or younger adults who have suffered terrible falls or have brain injuries/neurological disorders, you can rely on the original Barthel Index, a modified version, or even a translated version to help you gather evidence-based measurements and inform your treatment plans (e.g., neurologic rehabilitation, post-surgery recovery plans).
## **How to use the Barthel Index**
The Barthel ADL Index is a helpful tool to assess a person's physical function and ability to manage daily activities without assistance. It can even be used as a self-report measure, but the interpretation and clinical decisions still have to be made by a specialist. The following are the steps on how you can maximize this resource:
### **Step 1: Understand the purpose and components**
The Barthel Index is widely used to measure disability and assess functional independence in ADLs. It consists of 10 items: personal hygiene, bathing, feeding, toilet use, dressing, bowel control, bladder control, transfers, mobility on level surfaces, and stair climbing.
### **Step 2: Prepare for assessment**
Download the Barthel Index template from Carepatron by clicking the "Use template" button. This allows you to customize our Barthel Index template for your practice. For a PDF copy, you can also click "Download." Next, gather other necessary materials, such as a pen or pencil, and any assistive devices the patient typically uses. Ensure the assessment takes place in a quiet and comfortable environment. Introduce the purpose of the assessment to the patient and obtain their consent for the direct observation process.
### **Step 3: Conduct the assessment**
Observe the patient performing each ADL task or rely on self-report or caregiver input if direct testing is impossible. It's also important to note the activities that the patient can accomplish while carrying aid to assist them. When scoring each item, this ordinal scale typically ranges from 0 to 10, with some items having a maximum score of 15. The scoring criteria should be followed accurately to ensure consistency in assessment.
### **Step 4: Calculate the total score**
Add up each item's scores to obtain the total BI score. The maximum score is 100, indicating complete functional independence. Lower scores indicate varying degrees of dependence.
### **Step 5: Interpret and document the results**
Interpret the total BI composite score based on established guidelines included in the template. Document the outcome measures in the patient's medical record, including the total score range, individual item scores, and any relevant observations or comments. Use the BI score and other clinical assessments to guide care planning, discharge planning, and treatment decisions, especially in stroke recovery.
## **Scoring and interpretation**
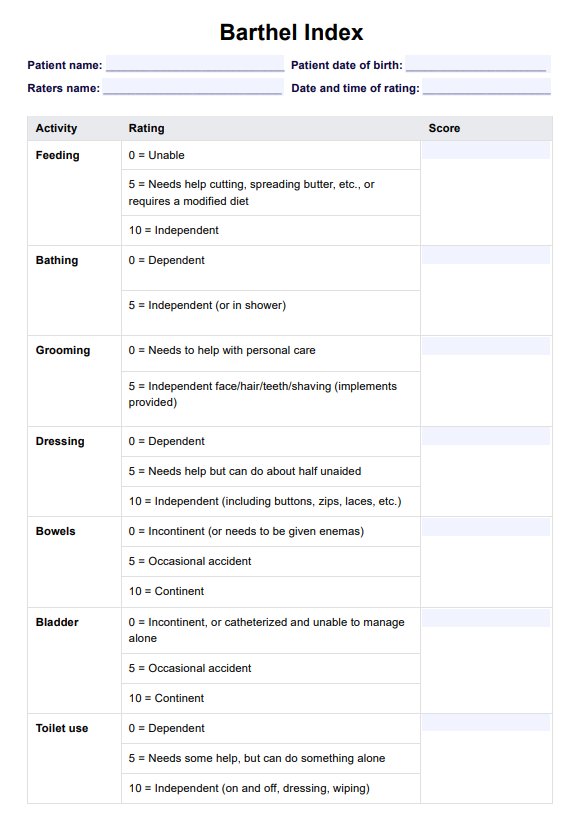
The Barthel Index's scoring system is designed to evaluate the patient's functional abilities objectively. As mentioned, the BI consists of 10 items, each scored on a scale ranging from 0 to either 10 or 15 points, depending on the specific task. The scoring criteria for each item are as follows:
- **Feeding**: 0 (unable), 5 (needs help), 10 (independent)
- **Bathing**: 0 (dependent), 5 (independent)
- **Grooming**: 0 (needs to help with personal care), 5 (independent)
- **Dressing**: 0 (dependent), 5 (needs help), 10 (independent)
- **Bowel control**: 0 (incontinent), 5 (occasional accident), 10 (continent)
- **Bladder control**: 0 (incontinent), 5 (occasional accident), 10 (continent)
- **Toilet use**: 0 (dependent), 5 (needs some help), 10 (independent)
- **Transfers (bed to chair and back**): 0 (unable, no sitting balance), 5 (major help), 10 (minor help), 15 (independent)
- **Mobility (on level surfaces)**: 0 (immobile), 5 (wheelchair independent), 10 (walks with the help of one person), 15 (independent)
- **Stairs**: 0 (unable), 5 (needs help), 10 (independent)
The total BI score is calculated by summing the individual item scores, with a maximum possible score of 100, indicating complete independence in ADLs. Individual items will also give you an idea about your patients, such as "is assistance required for this specific activity" and "they have difficulties controlling bowels and bladder, but are independent in other ADLs." This will inform your treatment plans, like determining what physical medicine is appropriate, what rehabilitation exercises should be implemented, etc.
## **Other tools for assessing functional independence**
Now, while it's safe to say that the Barthel Index has gone through validation studies and is determined to be a great disability scale with reliable diagnostic accuracy, structural validity, concurrent validity, and various other measurement properties (e.g., adequate floor effects, excellent ceiling effects), it would be best to also use other assessments to make sure you have consistent results when assessing patients.
Though D.T. Wade and C. Collin (1988) would disagree in doing so since "the temptation to use variations on the standard Barthel Index should be resisted," using other assessments will help you cover more ground. Here are examples of what you can use:
- **Functional Independence Measure**: The [Functional Independence Measure](https://www.carepatron.com/templates/functional-independence-measure) is often used alongside the Barthel Index. It was also subject to validation studies alongside it. It's an 18-item assessment tool that evaluates a patient's level of functional independence in self-care, mobility, communication, and social cognition. It has two subscales: the FIM motor subscale and the FIM cognitive subscale. This goes beyond just ADLs and covers thinking and memory, which also influence a person's everyday life. You will rate them between 1 to 7 during the time they're admitted into your facility, time of discharge, and follow-ups after discharge.
- **Berg Balance Scale**: The [Berg Balance Scale](https://www.carepatron.com/templates/berg-balance-scale) is meant to be used on elderly patients. The purpose of this scale is to assess their balancing capabilities and risk of falling. It has 14 items. You rate your patient from 0 to 4 based on balancing prompts. While this doesn't exactly measure ADLs per se, balance is a key part of certain activities of daily living, so if they have poor balance, they might have difficulty in performing ADLs such as taking a bath, getting dressed, simply moving, or even transferring themselves from bed to chair, vice-versa.
- **Modified Barthel Index**: The [Modified Barthel Index](https://www.carepatron.com/templates/modified-barthel-index) works the same way as the regular one. The only change is that there are more options to account for incremental improvements in a patient's functional status and capability to handle ADLs. You have more rating options with this version of the tool, and they might give you a better picture of your patient than the regular one, though we recommend using both for consistency.
- **Modified Rankin Scale**: The [Modified Rankin Scale](https://www.carepatron.com/templates/modified-rankin-scale-mrs) is a tool that's used to assess patients who've had a stroke. You only have to rate the patient between 0 to 6 based on your observations of them. This rating is an overall impression of the patient's capabilities post-stroke. The higher the rating, the more severe the disability, with a rating of 6 indicating that the patient is dead.
## **References**
Castiglia, S. (2017b). The culturally adapted Italian version of the Barthel Index (IcaBI): assessment of structural validity, inter-rater reliability and responsiveness to clinically relevant improvements in patients admitted to inpatient rehabilitation centers. Functional Neurology, 32(4), 221. https://doi.org/10.11138/fneur/2017.32.4.221
Liu, C., McNeil, J. E., & Greenwood, R. (2004). Rehabilitation outcomes after brain injury: disability measures or goal achievement? Clinical Rehabilitation, 18(4), 398–404. https://doi.org/10.1191/0269215504cr741oa
Mahoney, F. I., & Barthel, D. W. (1965). Functional evaluation: The Barthel Index. Maryland State Medical Journal, 14, 61–65.
Rollnik, J. D. (2011). The Early Rehabilitation Barthel Index (ERBI). Die Rehabilitation, 50(06), 408–411. https://doi.org/10.1055/s-0031-1273728
Wade, D. T., & Collin, C. (1988). The Barthel ADL Index: A standard measure of physical disability? International Disability Studies, 10(2), 64–67. https://doi.org/10.3109/09638288809164105
Commonly asked questions
Yes, the Barthel Index (BI) scoring can be considered relatively objective. The BI uses a standardized scoring system with clear criteria for each item, ranging from 0 (completely dependent) to 10 or 15 (completely independent). However, it is essential to note that the assessment still requires some subjective judgment, especially when observing the patient's performance or relying on self-report or caregiver input.
The Barthel Index is widely used to assess functional independence in activities of daily living (ADLs) across a variety of clinical settings and patient populations, including stroke patients, patients with musculoskeletal disorders, brain injuries, mental disorders, and multiple sclerosis. This can also be helpful in hospital discharge planning and nursing home care.
Functional assessment tools like the Barthel Index (BI) are commonly used to monitor functional status in patients, especially those with chronic stroke. It is typically administered multiple times, such as at admission, during treatment, and at discharge, to track changes in functional abilities and determine the level of assistance required. Repeated use of the BI is reliable and responsive to changes in functional status, making it an effective tool for assessing progress over time. While a single administration of the BI can provide valuable insights, it is generally recommended to use it regularly to accurately monitor the patient's functional trajectory and guide treatment decisions.