## **What is chest pain?**
Chest pain refers to any discomfort, pressure, tightness, or pain felt in the chest area. It can range from mild and fleeting to severe and life-threatening. Clinically, chest pain can arise from multiple structures in the thorax, including the heart, lungs, esophagus, muscles, bones, or chest wall, making it one of the most complex symptoms to evaluate.
From a cardiovascular standpoint, chest pain is most often linked to heart disease or coronary artery disease (CAD), where reduced blood flow to the heart muscle leads to angina pectoris or a myocardial infarction (heart attack). Patients commonly describe angina symptoms as pressure, squeezing, or burning pain in the center of the chest that can radiate to the jaw, neck, shoulder, or left arm. When triggered by exertion and relieved by rest or nitroglycerin, the episode is typically stable angina; if pain persists or worsens at rest, it may be unstable angina, requiring emergency care. Immediate treatment focuses on restoring blood flow and preventing further cardiac injury.
However, not all chest pain is cardiac in origin. Noncardiac chest pain can result from the lungs, gastrointestinal tract, or musculoskeletal system. Pulmonary causes such as a blood clot (pulmonary embolism) or pneumothorax often cause sharp chest pain that worsens with deep breathing or coughing. Gastroesophageal reflux disease (GERD) may produce a burning pain behind the sternum, while muscle strain or costochondritis can cause localized tenderness in the chest wall.
Because chest pain symptoms can signal conditions ranging from mild irritation to life-threatening emergencies, rapid evaluation is vital. Warning signs should prompt immediate action. Patients experiencing these symptoms should call their local emergency number without delay.
According to the American Heart Association (AHA) and the National Institute for Health and Care Excellence (NICE), early diagnosis and treating chest pain promptly, especially when related to reduced blood flow or high blood pressure, can significantly improve patient outcomes and reduce mortality (American Heart Association, 2025; Smeeth et al., 2010).
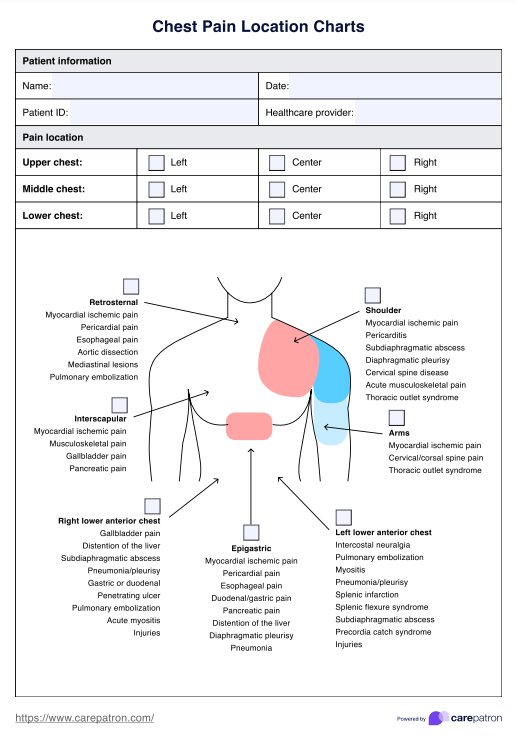
## **What is a Chest Pain Location Chart?**
A Chest Pain Location Chart is a clinical assessment tool used to help identify the potential source of chest discomfort by mapping where a patient feels pain. It allows patients to indicate precisely where their pain occurs and, in some cases, how it radiates to nearby regions such as the arm, jaw, neck, or upper abdomen.
By visualizing the location of the pain, the chart helps clinicians make early distinctions about the causes of chest pain. For instance, pain centered behind the sternum that radiates to the left arm or jaw may indicate a cardiac event such as angina, acute coronary syndrome (ACS), or myocardial infarction. Pain that worsens with breathing or coughing may suggest pleuritic or pulmonary conditions. In contrast, localized tenderness or pain aggravated by movement can indicate musculoskeletal issues, such as costochondritis or rib fractures.
In emergency and primary care settings, this chart can streamline triage and guide diagnostic priorities. When patients present with acute chest pain, quickly identifying the area and nature of discomfort helps clinicians decide whether immediate interventions, such as ECGs, cardiac enzyme testing, or imaging, are warranted. This chart also supports ongoing patient monitoring by tracking changes in pain patterns over time, helping clinicians assess treatment response and detect symptom progression early.
Despite its usefulness, the Chest Pain Location Chart has limitations. It offers a starting point for investigation rather than a definitive diagnosis. Because chest pain can be referred from other regions or present atypically, especially in older adults, women, or people with diabetes, location alone cannot confirm the cause (Manistamara et al., 2021; Ramamoorthy et al., 2021). The chart must always be used in conjunction with a thorough history, physical examination, and diagnostic testing, such as ECGs, chest imaging, and laboratory analyses.
## **How to use the Chest Pain Location Chart**
The Chest Pain Location Chart is a valuable diagnostic tool in healthcare. Here's a step-by-step guide on how to utilize this chart effectively:
### **Step 1: Access the template**
First off, access the template on the Carepatron app by clicking "Use Template." You can customize the template on the app before printing or sharing. You can also download a non-customizable PDF version by clicking "Download."
### **Step 2: Decipher the nature of the pain**
Initiate the process by asking the patient to characterize their pain. It could be sharp, dull, stabbing, burning, or squeezing. You can also ask them to provide a more accurate description if none of the terms fit perfectly. Understanding the nature of the pain can offer significant insights into its potential cause.
### **Step 3: Pinpoint the pain**
Next, request the patient to indicate the exact location of their discomfort on the Chest Pain Location Chart. This may be easier if you have a printed copy or a mobile device that you can hand to the patient. If the pain extends or radiates to other areas, it's essential to mark these regions as well. The precise location can provide clues about what's triggering the pain.
### **Step 4: Note additional symptoms**
It's crucial to record any other symptoms that the patient might be experiencing alongside chest pain. These could range from shortness of breath and nausea to dizziness or fatigue. Determining the presence of these symptoms is vital in case the patient is experiencing life-threatening conditions that first manifest as acute chest pain.
### **Step 5: Do additional tests**
Once you and your patient have pinpointed the location of the pain, begin conducting other clinical tests to determine the true cause and nature of the pain. These may include physical examinations, blood tests, or imaging studies such as chest X-rays,electrocardiograms (EKG/ECG), or echocardiograms. These tests will let you see into the heart, lungs, blood vessels, and surrounding skeletal structures.
### **Step 6: Analyze the collected information**
Use the data gathered from the Chest Pain Location Chart and the other tests to help identify potential causes of chest pain. The specific location and type of pain, as well as other reported symptoms, can offer valuable insights that guide the diagnostic process.
## **Interpreting chest pain patterns**
Once you’ve helped your patient map their discomfort using the Chest Pain Location Chart and gathered related details, the next step is to interpret the findings. Recognizing characteristic pain patterns allows you to narrow down the likely underlying cause and determine which system—cardiac, pulmonary, gastrointestinal, or musculoskeletal—is responsible for the symptom.
### **Central or retrosternal pain**
Pain centered behind the sternum is often cardiac in origin. It may present as pressure, squeezing, or heaviness and is classically associated with angina pectoris or myocardial infarction. This discomfort can radiate to the left arm, shoulder, jaw, or neck and may be triggered by exertion or emotional stress. However, non-cardiac causes—such as esophageal spasm, reflux, or hiatal hernia—can mimic this pattern, particularly if the pain occurs after meals or when lying flat
### **Lateral or pleuritic pain**
Pain located on one side of the chest, especially if sharp or stabbing, often suggests involvement of the pleura or the musculoskeletal system. Pleuritic pain typically worsens with deep breathing, coughing, or movement, pointing to possible pulmonary embolism, pneumothorax, or pleurisy. If tenderness is localized and reproducible by palpation, the cause is more likely musculoskeletal, such as costochondritis, rib fracture, or intercostal strain
### **Epigastric pain**
Pain in the upper central abdomen may arise from gastrointestinal conditions like gastritis, GERD, or peptic ulcer disease. Still, it can also reflect inferior wall myocardial ischemia, particularly in women (Ramamoorthy et al., 2021), older adults, or diabetic patients (Manistamara et al., 2021). Because these populations frequently present with atypical cardiac symptoms, epigastric pain should never be assumed to be gastrointestinal without proper cardiac evaluation
### **Interscapular or upper back pain**
Pain radiating to or centered between the shoulder blades can signal aortic dissection, gallbladder disease, or referred diaphragmatic pain. In aortic dissection, patients may describe the pain as “tearing” or “ripping,” often accompanied by sudden onset, hemodynamic instability, or pulse deficits—signs that require immediate emergency evaluation (Levy & Le, 2023).
### **Localized, reproducible pain**
When chest pain is localized and worsens with pressure, movement, or specific body positions, it is typically musculoskeletal in origin. Conditions such as costochondritis, sternoclavicular arthritis, or myofascial strain are common culprits. These cases are typically benign, but it’s still important to rule out overlapping causes, especially in patients with cardiac risk factors (Cleveland Clinic, 2024).
Always correlate pain distribution, including jaw pain, arm pain, or discomfort radiating to the neck or back, with vital signs, ECG findings, and risk factors before concluding. Many life-threatening conditions overlap in presentation, so when in doubt, manage chest pain as potentially cardiac until proven otherwise.
## **References**
American Heart Association. (2025, January 30). Angina (chest pain). https://www.heart.org/en/health-topics/heart-attack/angina-chest-pain
Levy, D., & Le, J. K. (2023). Aortic Dissection. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK441963/
Manistamara, H., Sella, Y. O., Apriliawan, S., Lukitasari, M., & Rohman, M. S. (2021). Chest pain symptoms differences between diabetes mellitus and non-diabetes mellitus patients with acute coronary syndrome: A pilot study. Journal of Public Health Research, 10(2). https://doi.org/10.4081/jphr.2021.2186
Ramamoorthy, L., Joseph, N., & Satheesh, S. (2021). Atypical manifestations of women presenting with myocardial infarction at tertiary health care center: An analytical study. Journal of Mid-Life Health, 12(3), 219. https://doi.org/10.4103/jmh.jmh_20_20
Smeeth, L., Skinner, J. S., Ashcroft, J., Hemingway, H., & Timmis, A. (2010). NICE clinical guideline: chest pain of recent onset. British Journal of General Practice, 60(577), 607–610. https://doi.org/10.3399/bjgp10x515124