Benefits of using Medication Reconciliation Form templates
There are numerous benefits to using a Medication Reconciliation Form and the template of a med reconciliation form instead of making one from scratch. Here are some of them:
Keep information traceable
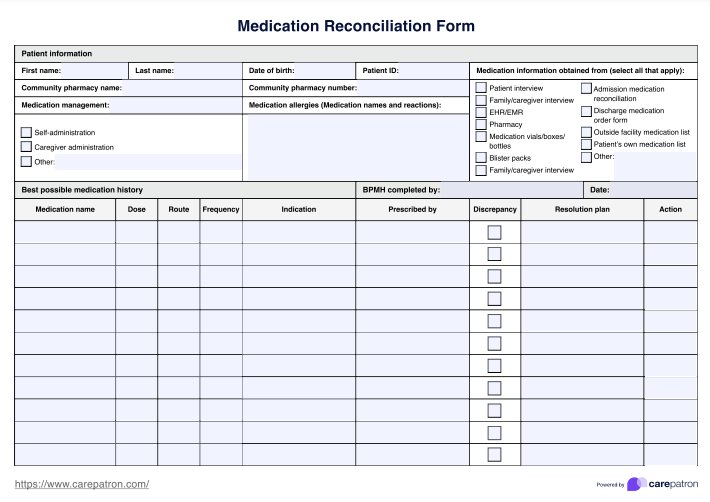
By including the names of the medications assessed, the sources used to create the BPMH, and the name and date of the BPMH creation, you can help improve your patients' medical records for the next time they transfer care.
Flowchart format
A medication reconciliation is more than a single table and involves several steps requiring careful attention. To help aid this process, we have created this Medication Reconciliation Form in a flowchart format - where medications are identified as to be started or continued in the BPMH flow onto the reconciled medication list.
Improve coordination of care
This tool will prove invaluable for improving your patient's care coordination. With a single, accurate source for your patient's current medications, all of those involved in your patient's care, including pharmacists, nurses, caregivers, and anyone else who treats your patient, will benefit.
Reduce medication errors
By identifying discrepancies in your patient's BPMH, you can prevent the error from propagating into your reconciled medication list. Within your multidisciplinary team, you can work on a solution to resolve these discrepancies and ensure the reconciled medication list is as error-free as possible, significantly reducing the risk of adverse drug events and improving overall medication safety.
Standardize the reconciliation process
Medication reconciliation processes should be conducted for every patient when transferring care to a new provider, service, or location. As such, you may have to become very familiar with this process, and having a standardized method of conducting these reconciliations will be an invaluable tool for you and your team.
Dedicated action section
When working within a team to solve complex problems, it can be easy for loose ends to go untied. To prevent this, there's a dedicated column in the template for selecting your chosen action. This ensures you have a plan for your patient, and no grey areas remain regarding their medication regime once the reconciliation process is complete.