Gluteal tendinopathy is one of the most common causes of chronic lateral hip pain, often resulting from repetitive mechanical loading or age-related tendon degeneration. Find out how targeted exercise programs, progressive loading, and adjunctive treatments can help restore tendon strength and function.
## **What is gluteal tendinopathy?**
Gluteal tendinopathy, often referred to as greater trochanteric pain syndrome, is a common cause of lateral hip pain. It primarily affects the gluteal tendons, which are the thick bands of tissue that connect the gluteal muscles (gluteus maximus, gluteus medius, and gluteus minimus) to the thigh bone. This condition typically manifests as pain and tenderness around the greater trochanter, the bony prominence outside the hip muscles. The gluteus medius muscle, in particular, is often implicated in this condition, as it plays a crucial role in stabilizing the pelvis during single-leg activities.
Gluteal tendinopathy often develops due to repetitive stress on the gluteal tendons, particularly during activities such as running, climbing stairs, or cycling (Grimaldi & Fearon, 2015; Pumarejo Gomez & Childress, 2021). Muscle imbalances or weakness in the hip and pelvic muscles, particularly in the gluteus medius, can increase strain on the tendons, potentially leading to injury. Additionally, poor biomechanics, direct trauma, or changes in gait patterns due to aging or pregnancy can contribute to the development of this condition.
Gluteal tendinopathy typically presents with lateral chronic hip pain localized around the greater trochanter. This pain, often described as a deep ache, tends to worsen with activities involving the hip abductors, such as walking, stair climbing, or lying on the affected side. Other symptoms include stiffness, a limited range of motion, and occasional swelling around the hip joint. These symptoms often develop gradually and may progress with repetitive activities or prolonged physical exertion.
## **Common exercises for gluteal tendinopathy**
Rehabilitation for gluteal tendinopathy emphasizes progressive loading to promote tendon remodeling, enhance gluteal muscle activation, and improve neuromuscular control around the hip. Current evidence identifies exercise-based therapy as the cornerstone of management, with structured strengthening programs shown to reduce pain and improve function more effectively than passive or injection-based interventions (Patrício et al., 2024).
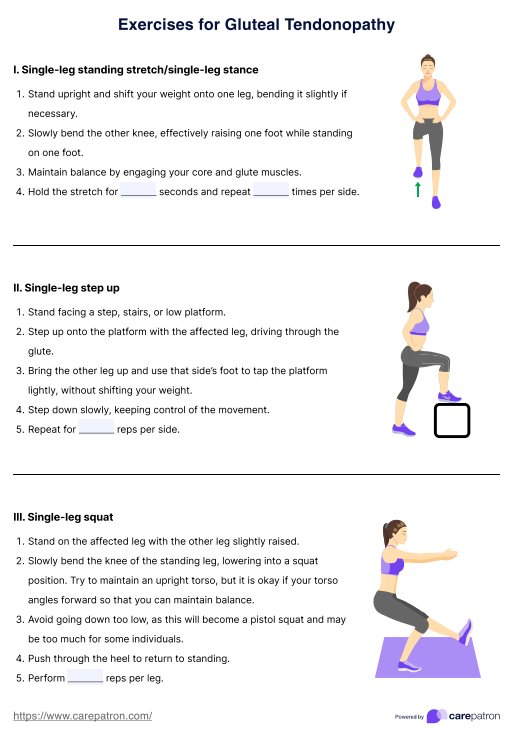
### **Single-leg standing stretch (single-leg stance)**
This exercise involves standing on one leg while keeping the knee slightly bent and engaging the core. It enhances single-limb balance, proprioception, and pelvic stability—key components in managing gluteal tendon overload. It also helps retrain the gluteus medius to maintain hip alignment during daily activities.
### **Single-leg step-up**
Performed by stepping onto a low platform with the affected leg and controlling the movement while stepping down. This exercise strengthens the gluteus maximus and medius through both concentric and eccentric loading, improving stair-climbing ability and lower-limb function.
### **Single-leg squat**
A partial squat on one leg that targets the gluteal and quadriceps muscles. It promotes tendon adaptation by increasing load tolerance and develops hip and knee control. This exercise is useful for restoring dynamic stability during walking, running, or functional tasks.
### **Prone leg lifts**
With the patient lying face down, one leg is lifted off the surface while keeping it straight and extended. This movement isolates the gluteus maximus and improves hip extension strength without compressing the lateral hip structures, making it ideal for early-stage strengthening.
### **Side-lying leg lifts**
In this exercise, the patient lifts the top leg upward while lying on one side of the body. It specifically targets the gluteus medius and minimus, helping restore lateral hip stability and reduce pelvic drop during gait. It is one of the most effective exercises for improving hip abductor endurance.
### **Standing leg raise**
Performed while standing upright and lifting one leg forward with control. This exercise promotes hip flexor and core engagement while reinforcing postural stability. It also complements gluteal training by enhancing overall lower-limb coordination and functional movement control.
## **How to use our Exercises for Gluteal Tendinopathy Handout**
Our Exercises for Gluteal Tendinopathy Handout provides clear instructions and visuals to guide you and your patients through exercises that target the affected muscles. Here's how you can integrate it effectively into your practice:
### **Step 1: Download the resource**
Click the "Use template" button to access a customizable version that allows you to modify, print, and fill out the handout. Alternatively, click the "Download" button to save a fillable and printable PDF version.
### **Step 2: Distribute the handout**
Introduce the handout to your patient, explaining its purpose and the benefits of consistent exercise. You can either give it to them as part of an in-person consultation or share it digitally for remote access.
### **Step 3: Guide the patient through the exercises**
Demonstrate each exercise, ensuring proper form and technique. Teach the patient how to adjust intensity and repetitions according to their progress. Use this opportunity to empower the patient to use the handout independently, fostering engagement in their recovery.
## **Other treatment options for gluteal tendinopathy**
While progressive exercise and patient education remain first-line management strategies, several adjunctive treatments may be considered depending on symptom severity, chronicity, and tissue status. These options are best integrated into a comprehensive plan that continues to emphasize gluteal tendinopathy exercises, strengthening exercises, as well as isometric and isotonic exercises for the hip and buttock area to maintain tendon strength and function.
### **Corticosteroid injections**
Research indicates that ultrasound-guided corticosteroid injections can provide short-term pain reduction in patients with gluteal tendinopathy (Ilizaliturri et al., 2022). However, multiple studies (Bremer et al., 2025; Mellor et al., 2018) have shown that benefits tend to diminish over time, with exercise and education outperforming corticosteroids at long-term follow-up. While injections may temporarily reduce pain to facilitate rehabilitation, repeated use can impair tendon healing and should be used judiciously.
### **Platelet-rich plasma (PRP) and other biologics**
For patients who fail conservative care, PRP shows promising benefits in some RCTs and reviews, with short-term functional gains versus corticosteroid injection. According to Fitzpatrick et al. (2019), improvements in pain and function are greater at 12 to 24 weeks compared to those with corticosteroid injections.
### **Extracorporeal shock wave therapy (ESWT)**
Shock wave therapy, either radial or focused, has demonstrated moderate success in improving pain and functional scores among patients with chronic tendinopathies. Research suggests it may promote tendon healing through neovascularization and collagen regeneration (Speed, 2014). While ESWT can be a valuable adjunct for patients resistant to loading programs, evidence remains mixed, and optimal treatment parameters are yet to be standardized.
### **Analgesics and adjunctive modalities**
Non-steroidal anti-inflammatory drugs (NSAIDs), heat or cold therapy, and activity modification may help manage pain and inflammation during the early stages of treatment. These interventions are recommended to complement, rather than replace, mechanical loading programs and are best used to support exercise adherence and adherence to mechanical loading programs.
### **Surgery (for refractory or structural tears)**
When persistent disability remains despite comprehensive nonoperative care, or when imaging confirms significant abductor tendon tearing, endoscopic or open repair with/without bursectomy or ITB procedures can improve pain and abductor strength. Reserve for carefully selected cases after failed conservative pathways.
## **References**
Bremer, T., Nicklen, P., Fearon, A., & Morrissey, D. (2025). The efficacy of gluteal tendinopathy treatments: A systematic review. Clinical Rehabilitation. https://doi.org/10.1177/02692155251327298
Fitzpatrick, J., Bulsara, M. K., O’Donnell, J., & Zheng, M. H. (2019). Leucocyte-Rich platelet-rich plasma treatment of gluteus medius and minimus tendinopathy: A double-masked randomized controlled trial with 2-year follow-up. The American Journal of Sports Medicine, 47(5), 1130–1137. https://doi.org/10.1177/0363546519826969
Grimaldi, A., & Fearon, A. (2015). Gluteal tendinopathy: Integrating pathomechanics and clinical features in its management. Journal of Orthopaedic & Sports Physical Therapy, 45(11), 910–922. https://doi.org/10.2519/jospt.2015.5829
Ilizaliturri, V. M., Zepeda Mora, R., & Rodríguez Vega, L. P. (2022). Rehabilitation after gluteus medius and minimus treatment. Arthroscopy, Sports Medicine, and Rehabilitation, 4(1), e41–e50. https://doi.org/10.1016/j.asmr.2021.10.024
Mellor, R., Bennell, K., Grimaldi, A., Nicolson, P., Kasza, J., Hodges, P., Wajswelner, H., & Vicenzino, B. (2018). Education plus exercise versus corticosteroid injection use versus a wait-and-see approach on global outcome and pain from gluteal tendinopathy: prospective, single-blinded, randomised clinical trial. BMJ, 361(361), k1662. https://doi.org/10.1136/bmj.k1662
Patricio, T., Bezerra, A., & Rodrigo Scattone Silva. (2024). Effects of exercise-based interventions on gluteal tendinopathy. Systematic review with meta-analysis. Scientific Reports, 14(1). https://doi.org/10.1038/s41598-024-53283-x
Pumarejo Gomez, L., & Childress, J. M. (2021). Greater trochanteric syndrome. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK557433/
Speed, C. (2014). A systematic review of shockwave therapies in soft tissue conditions: focusing on the evidence. British Journal of Sports Medicine, 48(21), 1538–1542. https://doi.org/10.1136/bjsports-2012-091961