


What is spinal shock?
Spinal shock is a temporary condition that occurs following a spinal cord injury, characterized by a loss of reflexes, motor function, and sensory function below the level of the injury. This phase can last from several hours to weeks and involves a complete absence of all neurological activity below the site of the injury.
This condition is critical to diagnose and manage promptly to prevent further complications and to initiate appropriate treatment and rehabilitation strategies.
Symptoms of spinal shock
Spinal shock presents with various symptoms, reflecting the severity and level of the injury.
- Flaccid paralysis and loss of muscle tone below the injury site
- Absence of reflexes in the affected areas
- Bradycardia (slowed heart rate) and hypotension (low blood pressure) due to loss of sympathetic tone
- Areflexia, which is the lack of response to stimuli
- Loss of sensation or sensory deficits below the injury level
- Bladder dysfunction
Causes of spinal shock
Spinal shock can result from various traumatic and non-traumatic events.
- Direct trauma to the spinal cord, such as from accidents or falls
- Surgical procedures involving the spine
- Infections and inflammation, such as transverse myelitis or spinal abscesses
- Disruption of blood flow to the spinal cord, such as from a spinal stroke
What is the Bulbocavernosus Reflex (BCR)?
The Bulbocavernosus Reflex (BCR) is a physiological reflex that involves the contraction of the bulbocavernosus muscle in response to stimulation of the glans penis in males or the clitoris in females. According to Previnaire (2018), this reflex helps assess the function of the sacral spinal cord segments (S2-S4).
During the initial phase of spinal shock, this reflex is typically absent due to the loss of all reflex activity below the level of the spinal cord injury. The return of the BCR as spinal shock resolves indicates the recovery of reflex activity and can help differentiate between upper motor neuron and lower motor neuron lesions. The presence of the BCR suggests that the reflex arcs in the sacral segments are intact, which is important for diagnosing the extent and nature of spinal cord injuries.
How is this test conducted?
The BCR test is performed by following the steps below:
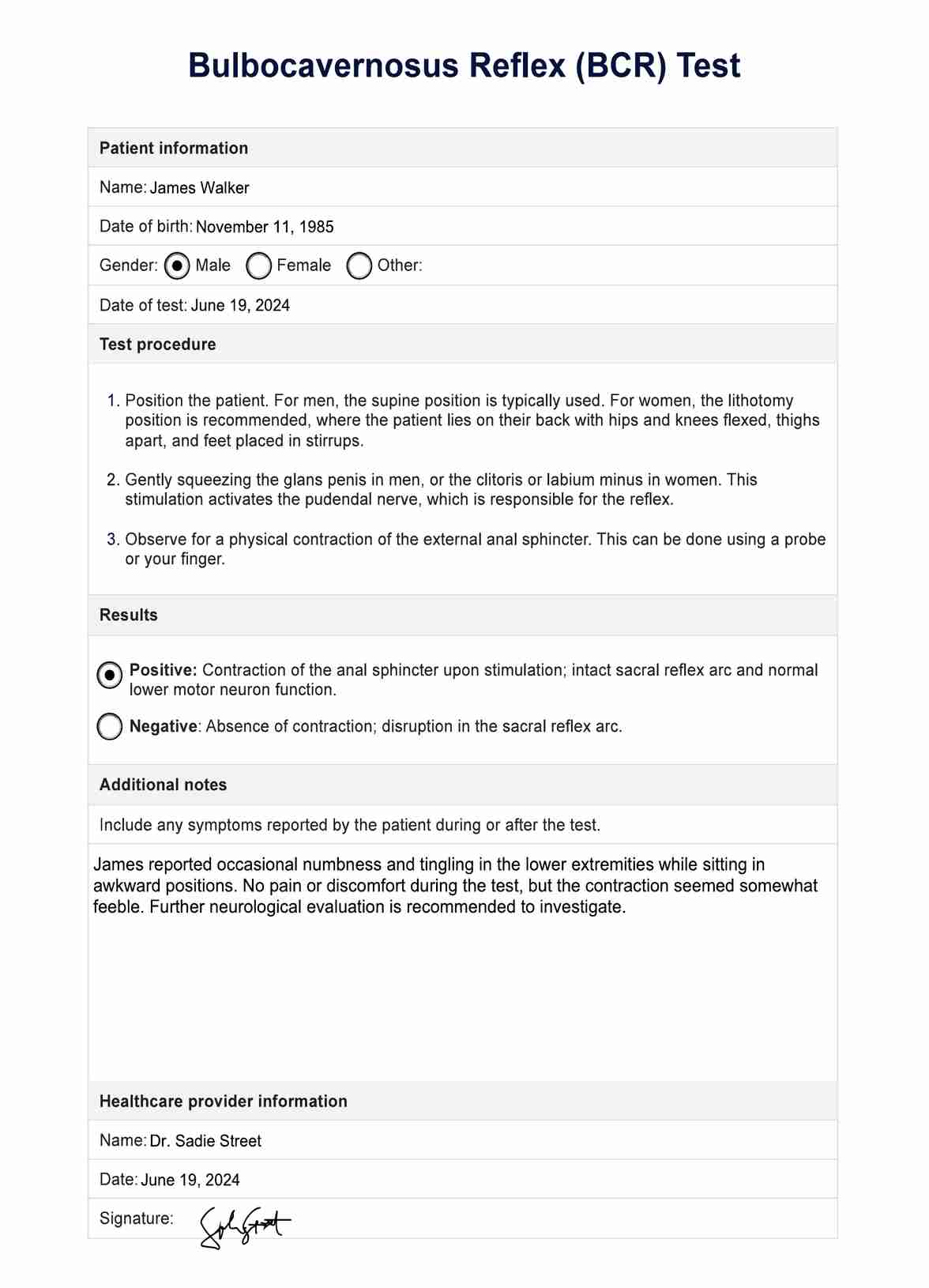
- Position the patient. For men, the supine position is typically used. For women, the lithotomy position is recommended, where the patient lies on their back with hips and knees flexed, thighs apart, and feet placed in stirrups.
- Gently squeezing the glans penis in men, or the clitoris or labium minus in women. This stimulation activates the pudendal nerve, which is responsible for the reflex.
- Observe for a physical contraction of the external anal sphincter. This can be done using a probe or your finger.
How are the results interpreted?
Interpreting the BCR test results helps assess the integrity of the sacral spinal segments. If you feel a contraction of the anal sphincter upon stimulation, it is a positive test, which indicates intact sacral reflex arcs, and is a sign of spinal cord integrity. In contrast, the absence of contraction equals a negative test, which suggests damage to the sacral segments/pathways or lower motor neuron lesions, which can indicate spinal cord injury or pathology.
Next steps after conducting this test
Following the BCR test, several steps may be necessary depending on the results. You may engage in further diagnostic testing, such as MRI or CT scans, to assess the extent of spinal cord damage. Comprehensive neurological evaluations also help to determine the level and severity of spinal cord injury. Lastly, you may start the development of a treatment plan, including physical therapy, medications, and possibly surgery, to manage the condition and improve patient outcomes.









