All-in-one EHR for every practitioner
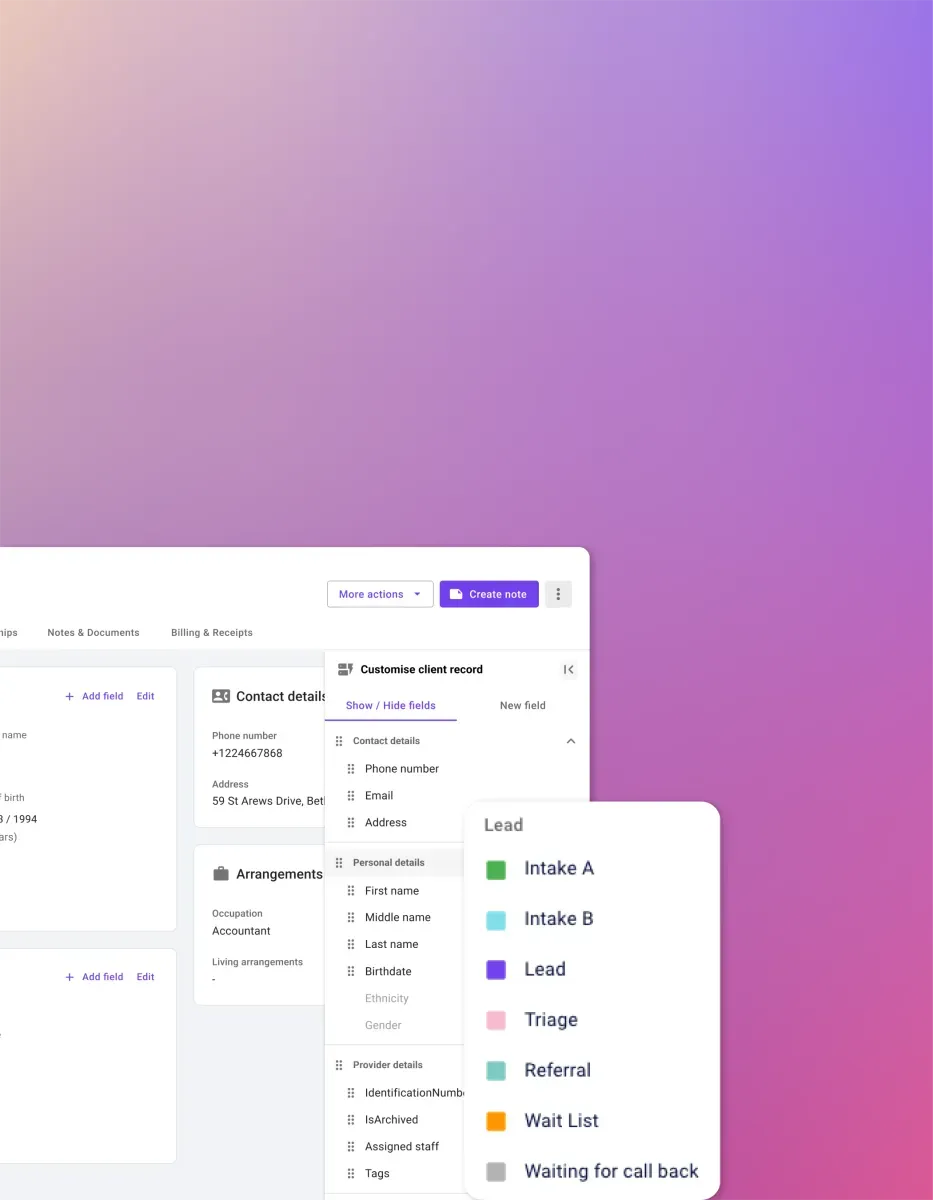
Carepatron's easy-to-use EHR software is designed to improve record management and save you time. Securely store documents, integrate with other tools, and simplify clinical documentation.




The free patient record software for your healthcare team
Advance your healthcare practice with Carepatron's unrivaled electronic health record software. Our HIPAA-compliant software ensures the utmost security, utilizing multiple layers of AES-256 encryption for confidential patient data.

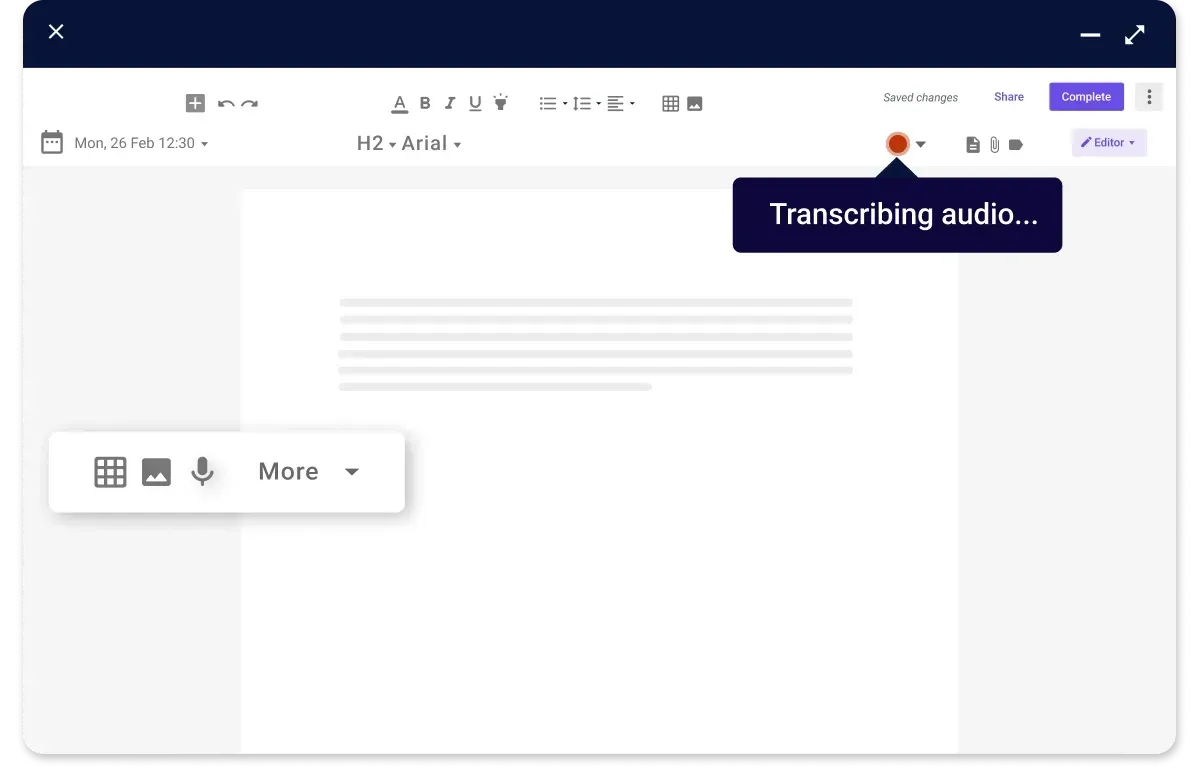
High-level integration
Carepatron's transcription tool seamlessly integrates with existing EHR systems and other healthcare software, facilitating smooth data transfer and ensuring that transcription is seamlessly incorporated into the existing workflow without disruption.
Carepatron’s electronic health records software
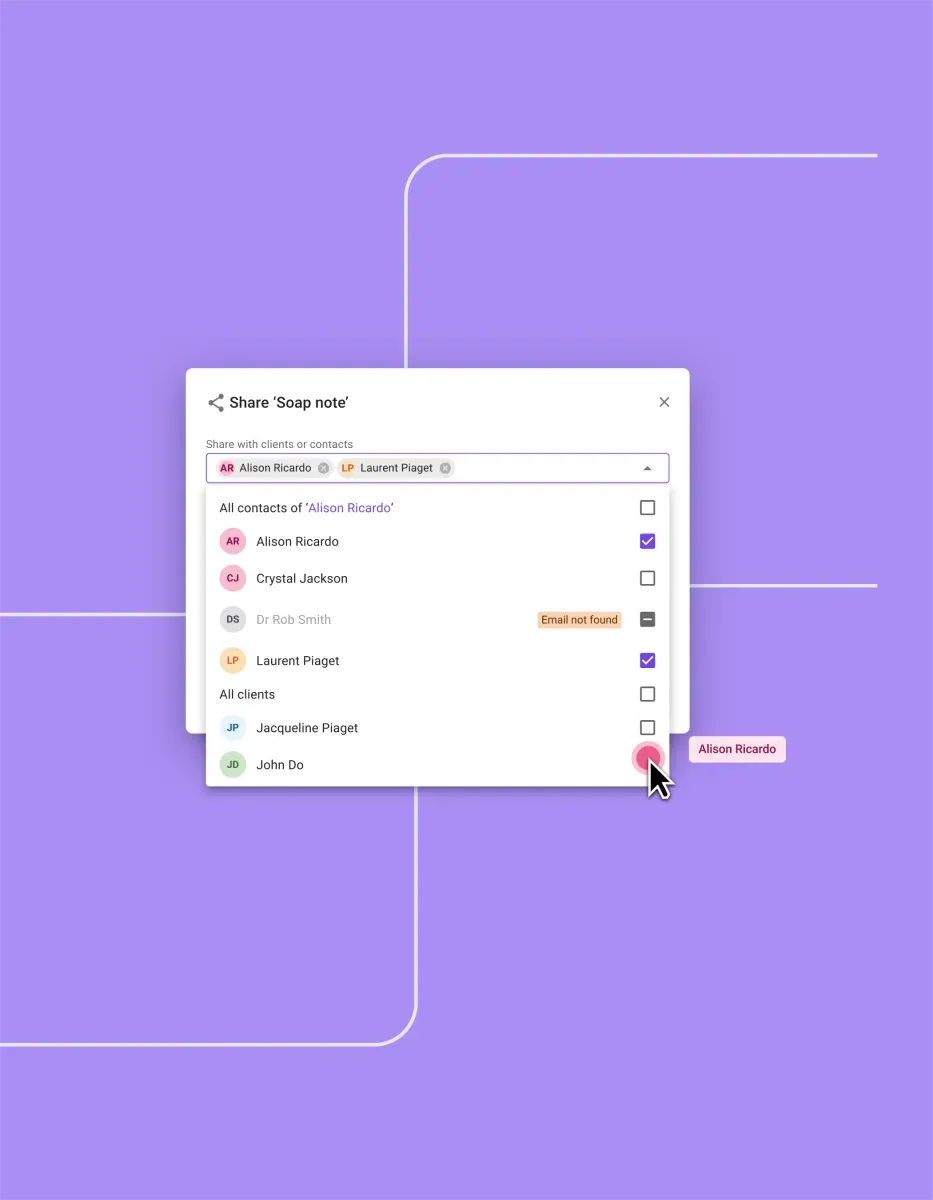
Carepatron's free patient record software offers a revolutionary approach to healthcare documentation. With robust features like HIPAA-compliant security and multiple clinical note formats, our free patient database will elevate your healthcare practice.

24/7 support
Our stellar support squad is here round-the-clock, every day of the week, ready to help you with any queries or concerns. Your satisfaction is our top priority as we strive to deliver an exceptional user experience.

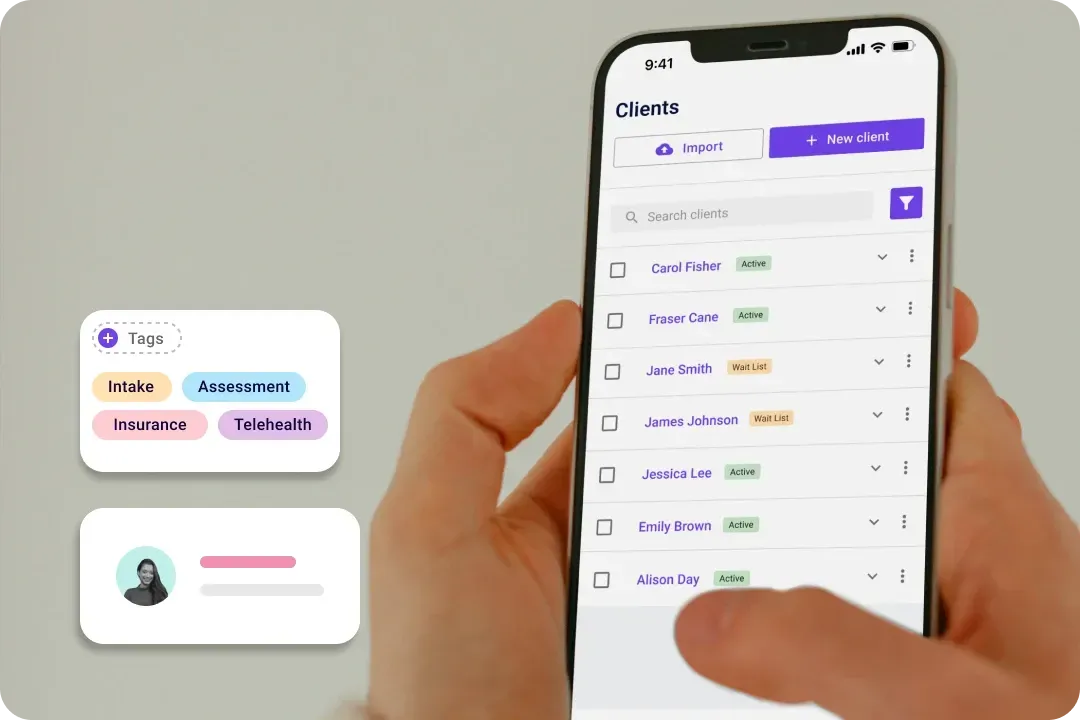
Access anytime
Whether via desktop or mobile, you can access our software anytime, anywhere. Never miss a beat, and stay on top of patient care with our user-friendly interface.
Trusted by more than 100,000 practitioners

"It’s so easy to connect with my staff"
CLAIRE, PHYSICAL THERAPIST

"Carepatron saves me 2 hours everyday"
AEGEUS L, HEALTH COACH

"My team loves how simple it is to use"
ANDREA MAGNUS, PRACTICE MANAGER
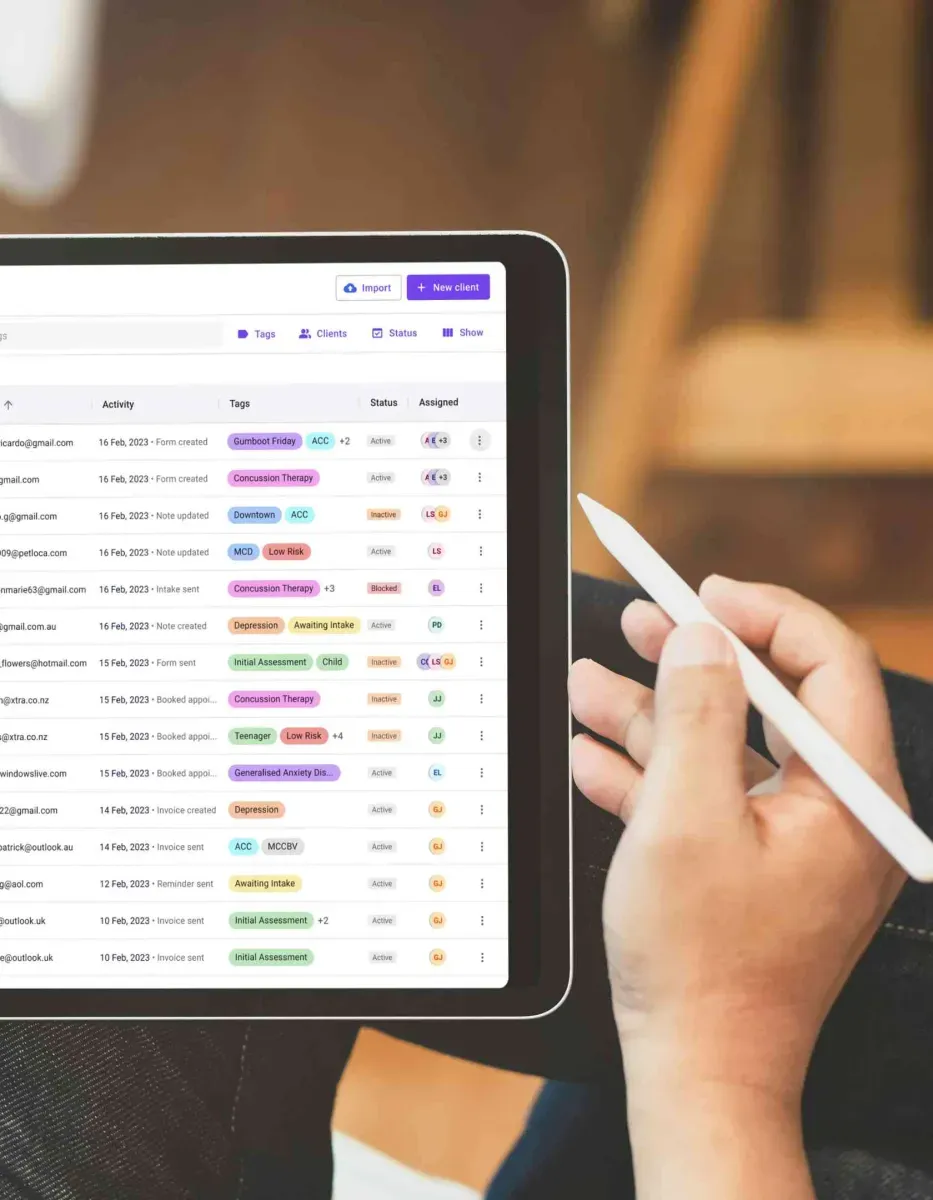
The benefits of using free patient record software
Unlock the power of free patient records software like Carepatron's EHR for unparalleled benefits. Enhance patient care and self-management through our free EMR with personalized access to medical data, fostering transparency and empowering patients in their health journey. Discover the advantages of leveraging free patient records software like Carepatron for enhanced healthcare management and efficiency. Here are its benefits:

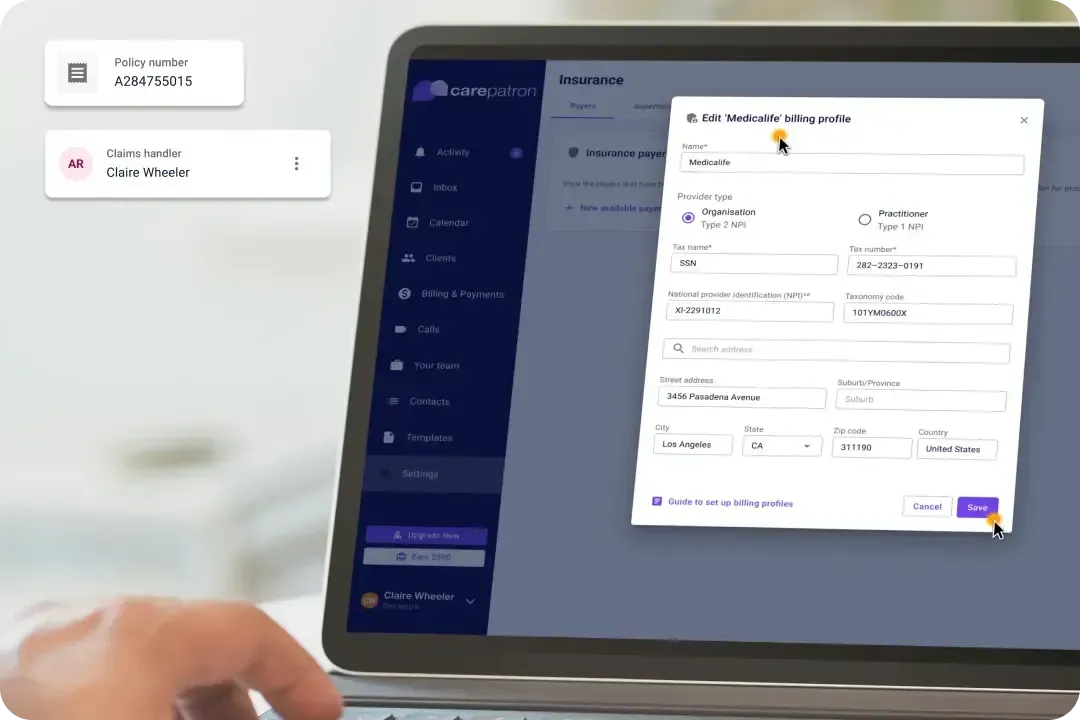
HIPAA-compliant security
Ensure patient data confidentiality with robust HIPAA-compliant security measures, including AES-256 encryption and secure cloud storage.

Patient portal integration
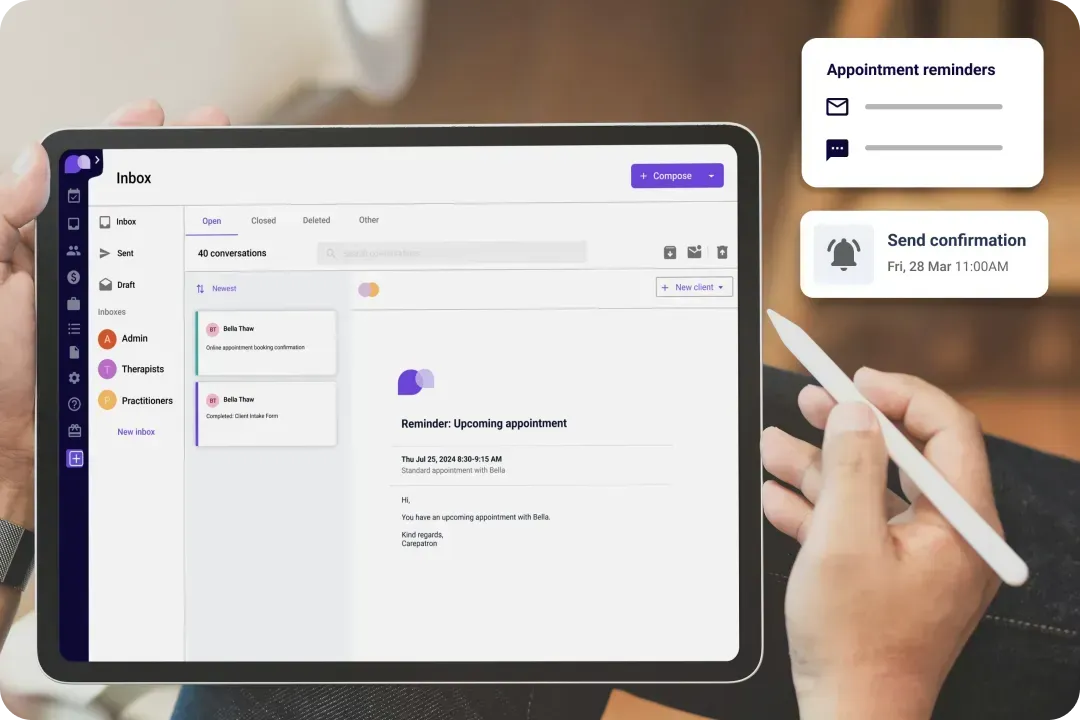
Empower patients with 24/7 access to their medical information and appointment details, promoting transparency and engagement in their healthcare journey.

Appointment workflow optimization
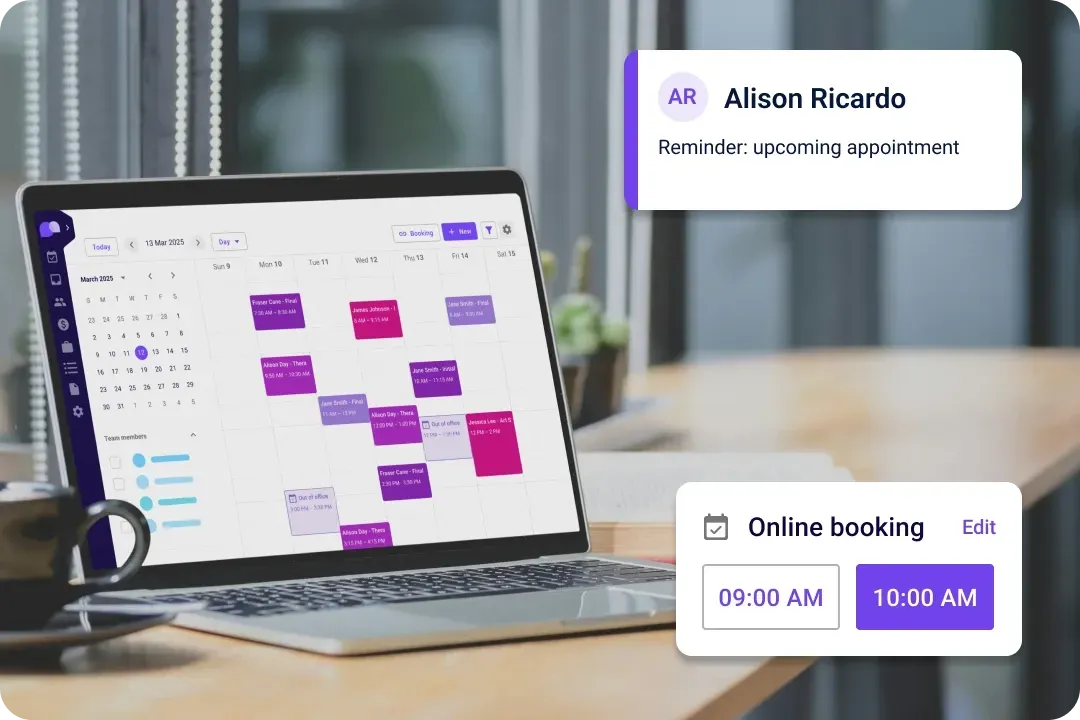
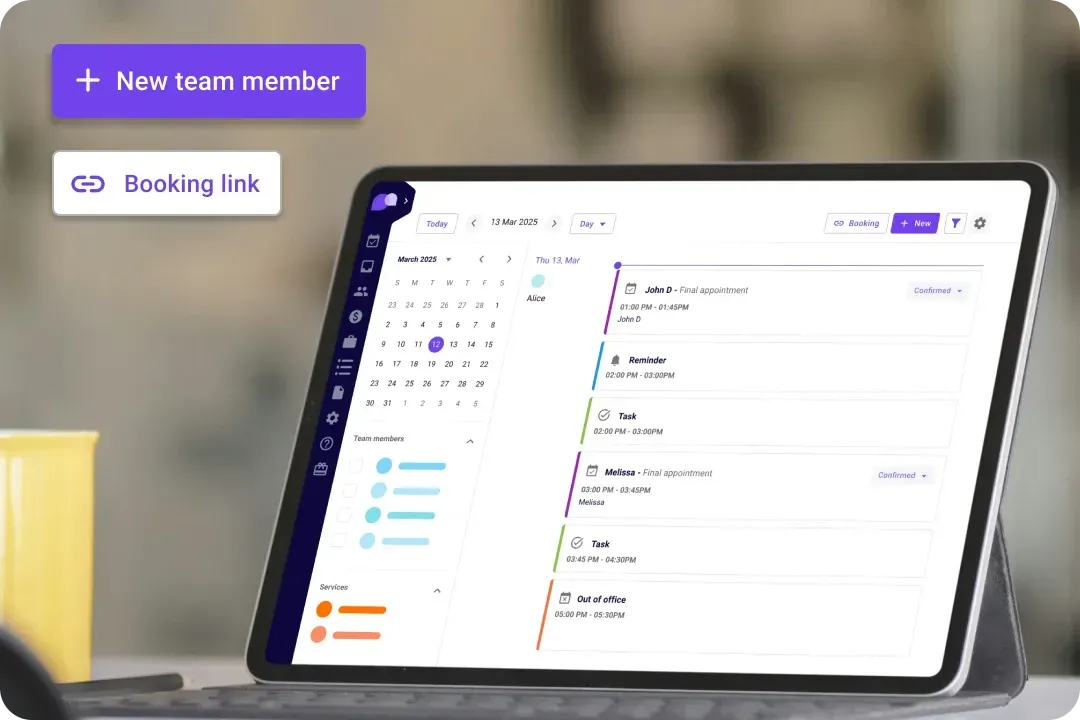
Maximize practice efficiency with integrated appointment scheduling software, allowing flexible scheduling and streamlined patient management.
The online electronic health records software for every healthcare team
Carepatron's online EHR software is tailored for every healthcare team. It provides free EMR capabilities and precisely caters to diverse fields.

Boost productivity and efficiency
Dive into a world of electronic clinical notes, automated scheduling, and telehealth features! Our software cuts through manual tasks, freeing up your time for what matters most – patient care.

Streamlined communication
Carepatron's health coaching app facilitates seamless communication among healthcare team members. Enhance collaboration, share insights, and coordinate care plans effortlessly, ensuring everyone is on the same page.

Efficient task management
Effortlessly distribute tasks among your team members utilizing our advanced physical therapy scheduling software. Stay organized and enhance collaboration by ensuring everyone is informed with real-time updates and seamless communication.

Secure data management
Safeguard patient information with robust encryption, ensuring compliance with the highest data protection standards. Our secure data management meets and exceeds industry benchmarks, providing a foundation of trust and confidence.
Brief breakdown: How to use our electronic health records software
Seamlessly manage patient information with our user-friendly free patient record software. Follow these steps to use this EHR software:

Nurses
Nurses can expedite note-taking processes, ensuring timely and accurate documentation of patient assessments, interventions, and responses for better care coordination.

Primary care physicians
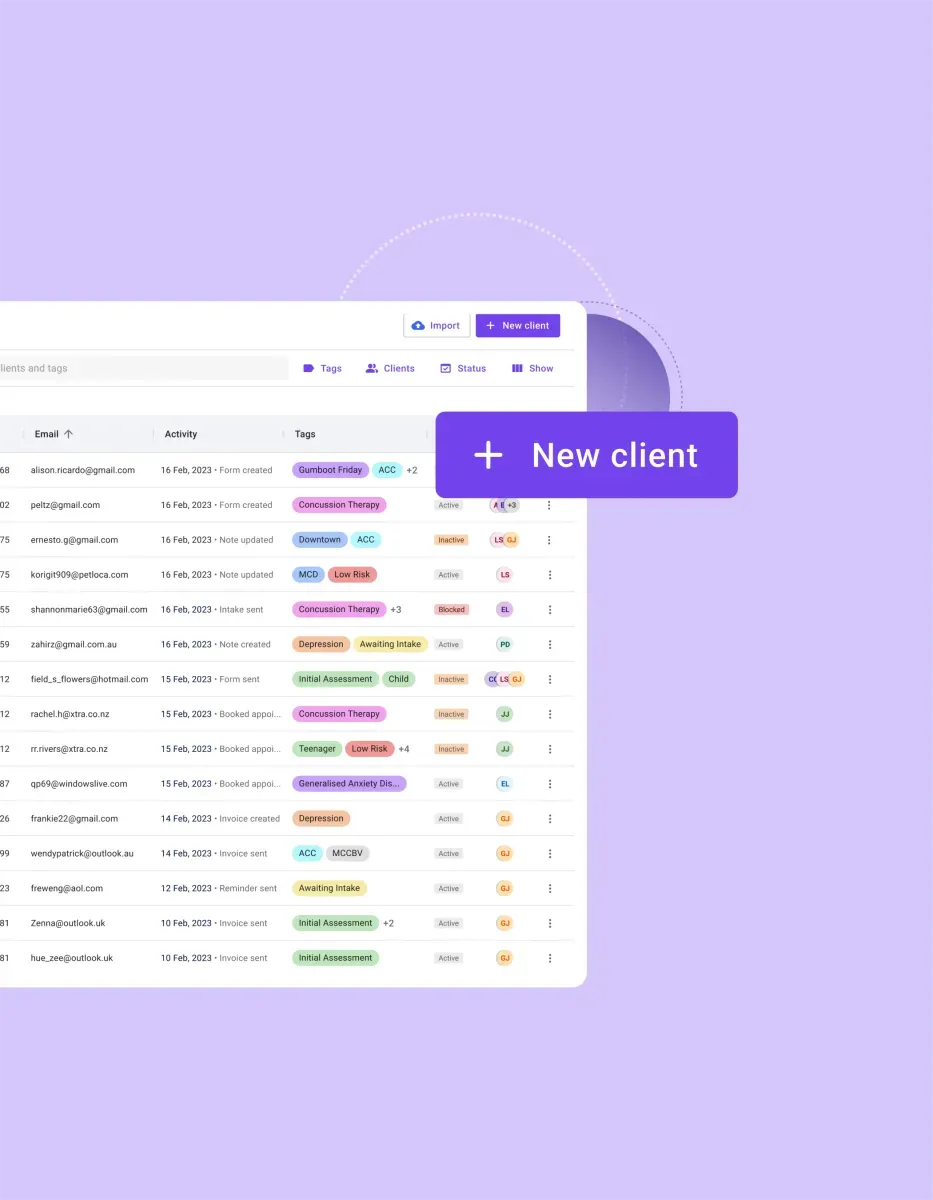
Online patient portals facilitate seamless access to comprehensive patient records. Primary care physicians can efficiently review medical history, lab results, and treatment plans, ultimately improving the quality of care delivered.


Frequently asked questions
EHR and practice management software
Get started for free
*No credit card required
Free
$0/usd
Unlimited clients
Telehealth
1GB of storage
Client portal text
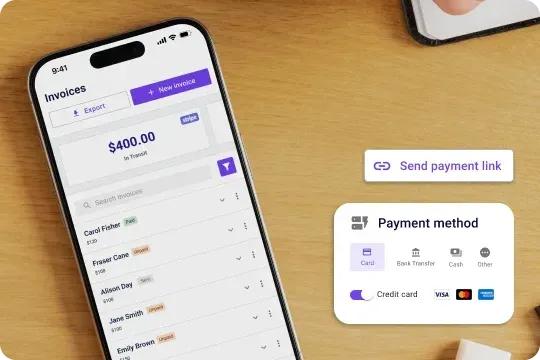
Automated billing and online payments