Fewer no-shows with automated reminders across Carepatron practices.
Star rating across 900+ reviews on Capterra and G2.
Saved per week on average by removing manual scheduling from your workflow.
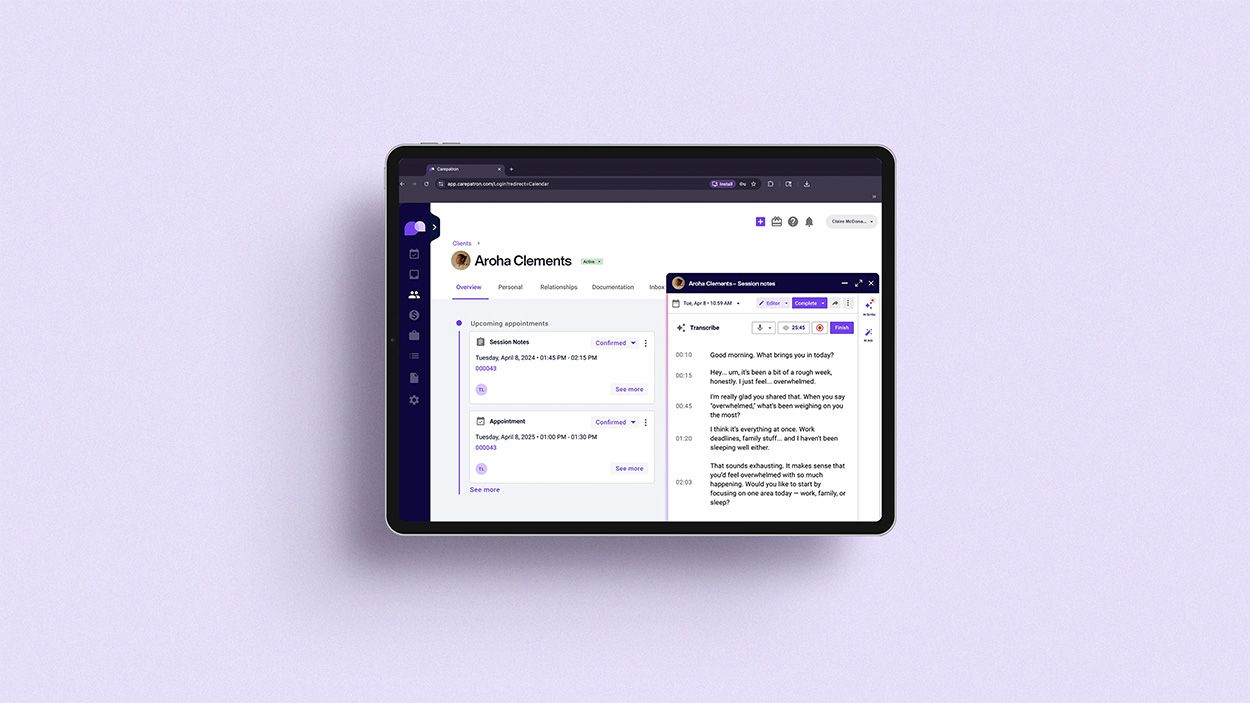
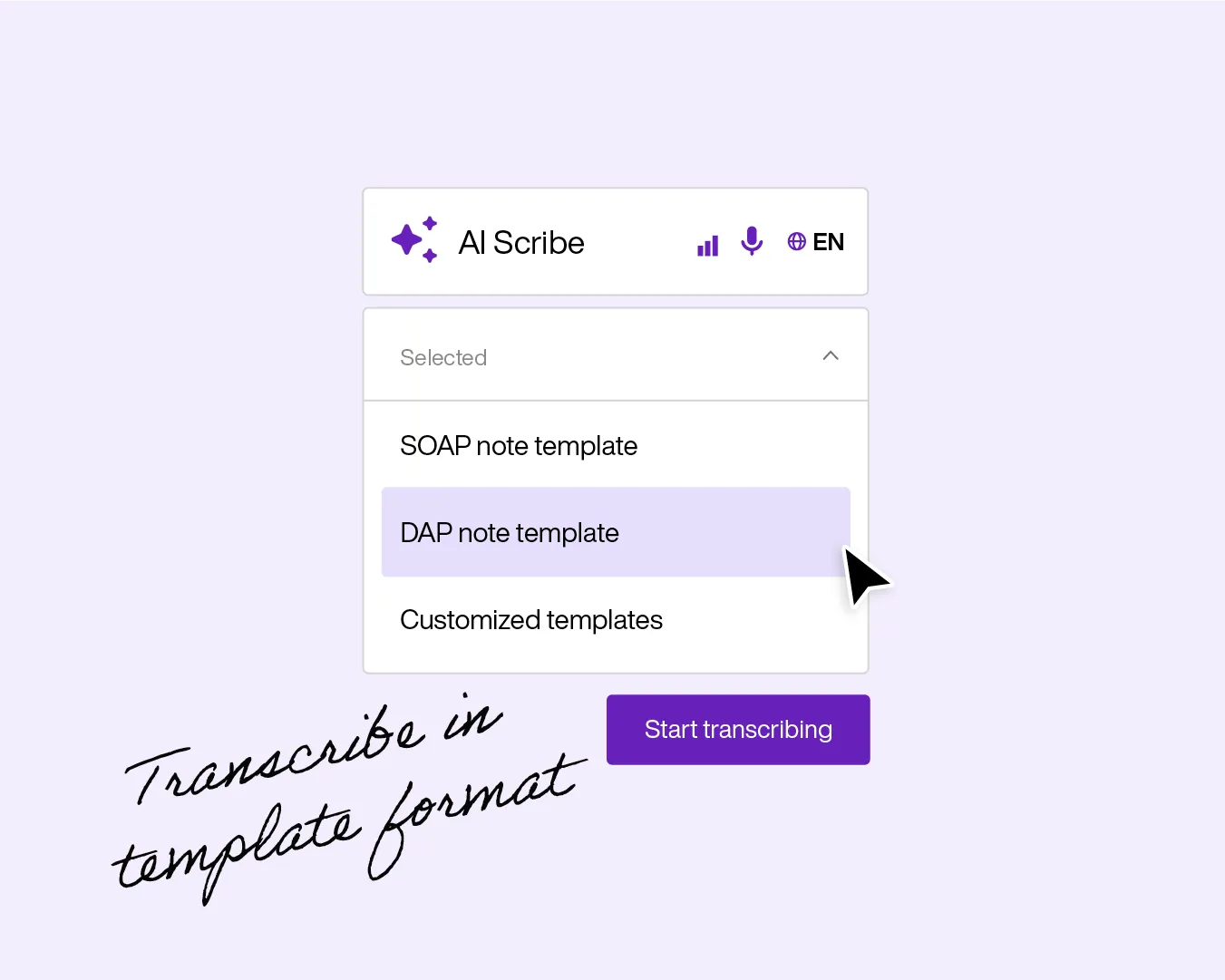
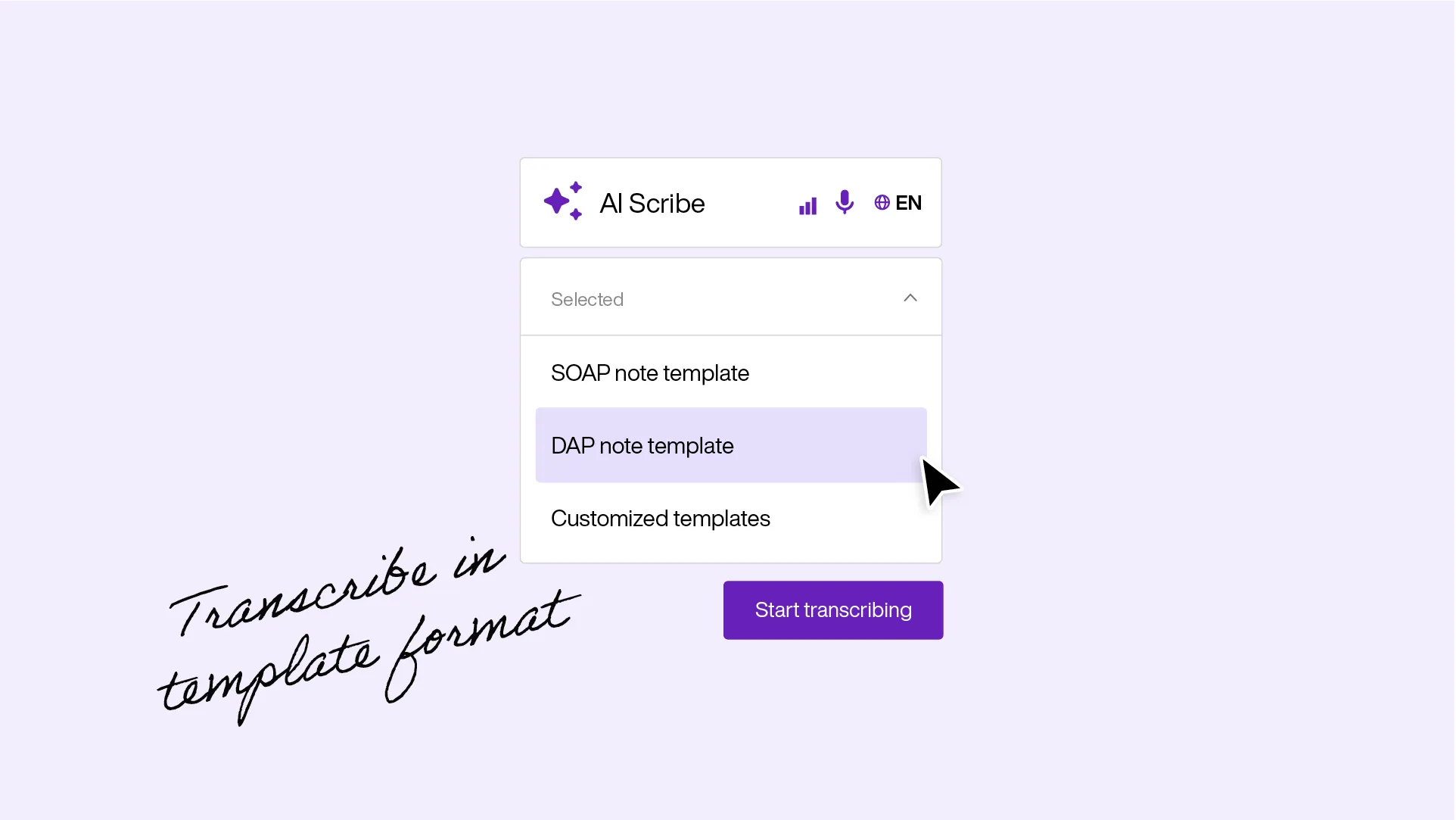
AI Scribe
You focus, we write
AI scribe transcribes the audio, then transforms it into your chosen clinical template. SOAP, DAP, BIRP, or your own format. Choose the writing perspective, the verbosity, even the output language. Review, edit, sign. Done.
- Transcription during sessions and dictation between them
- One-click formatting into any clinical note template
- Customisable language, perspective, and level of detail
Clinical notes
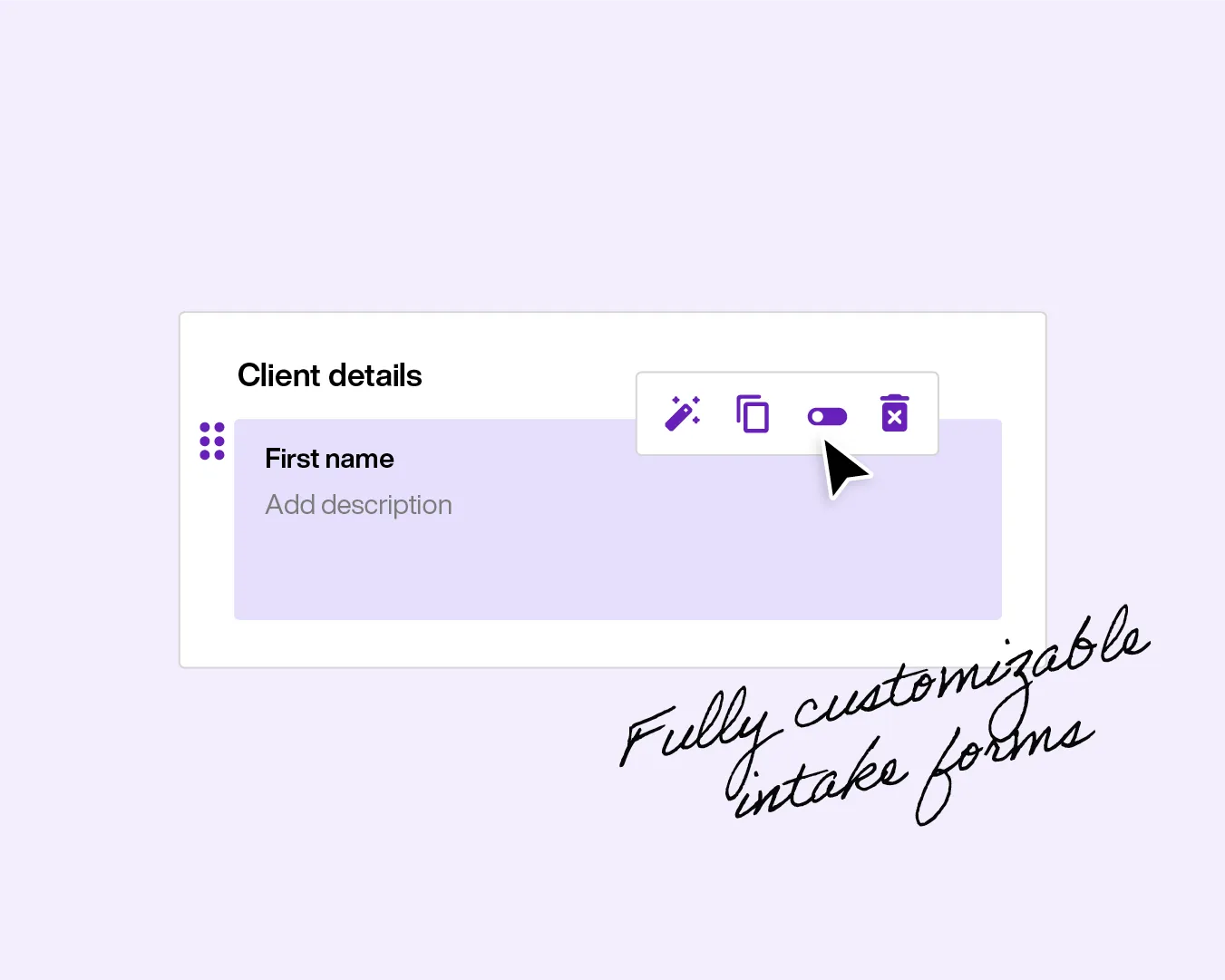
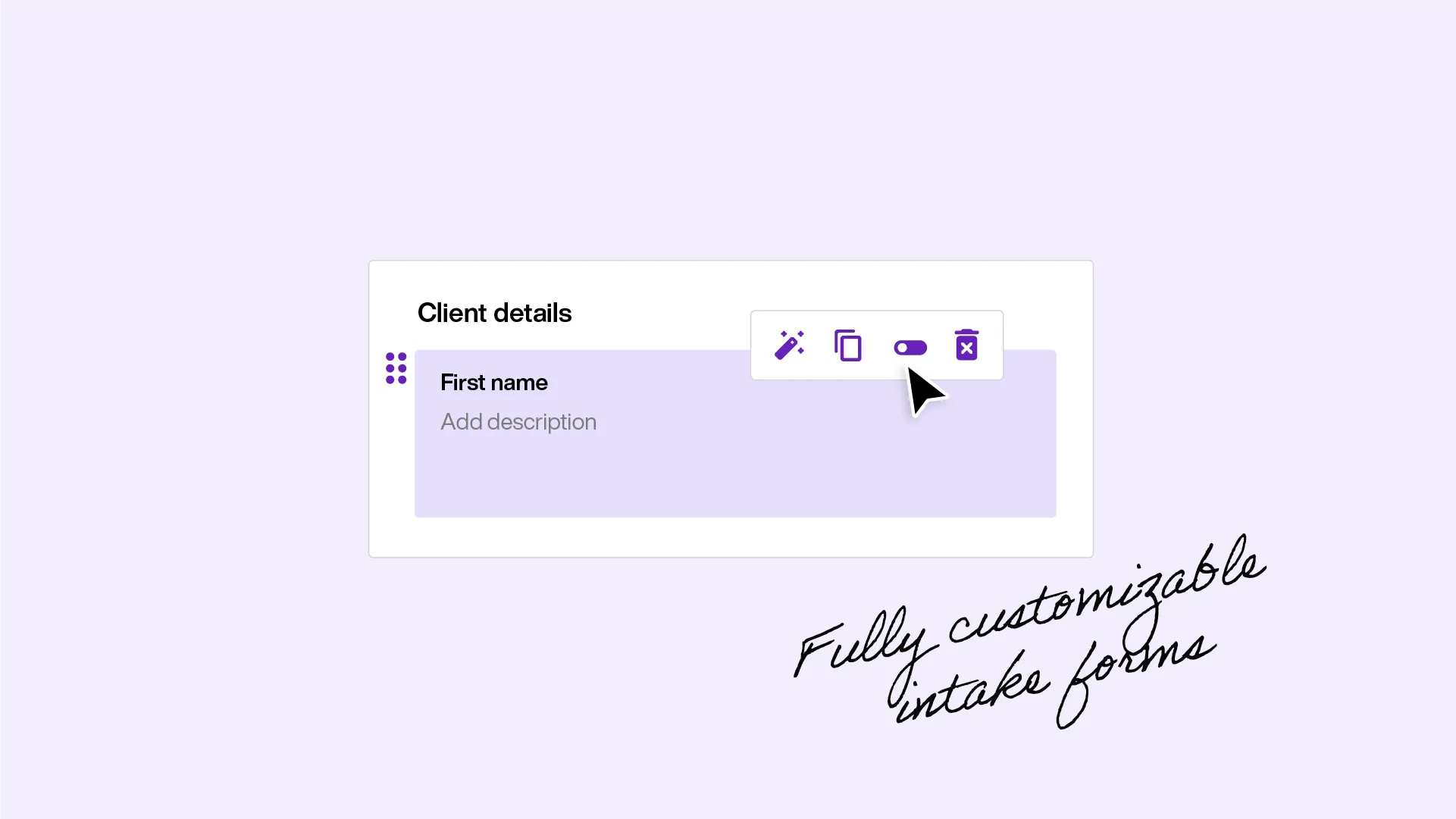
Templates for everything
Set default intake forms that send automatically when a client books. Build from scratch with pre-fill client information.
- Community template library across specialties and note types
- Fully customisable with form fields, section grids, and AI prompts
- Default intake forms sent automatically on booking
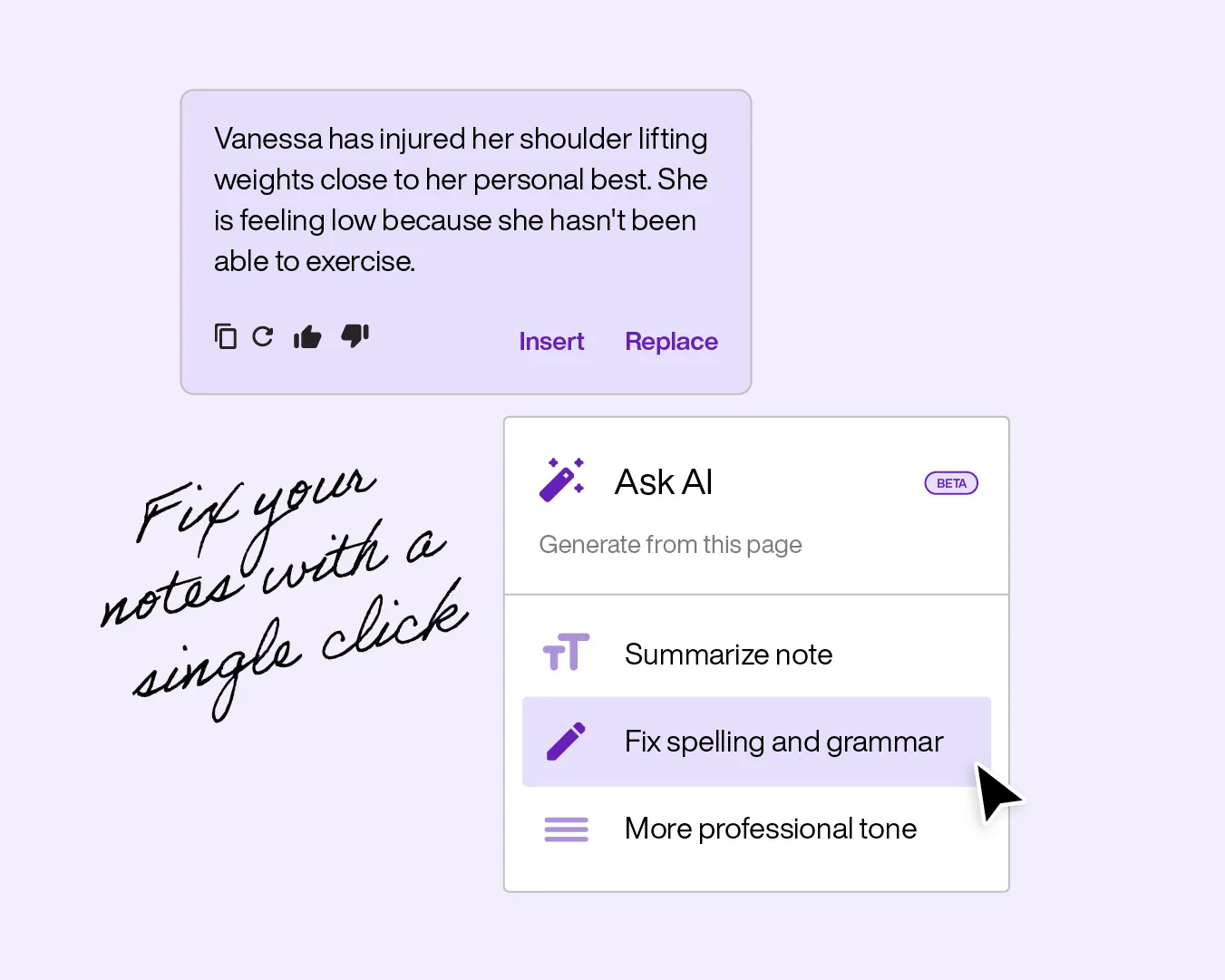
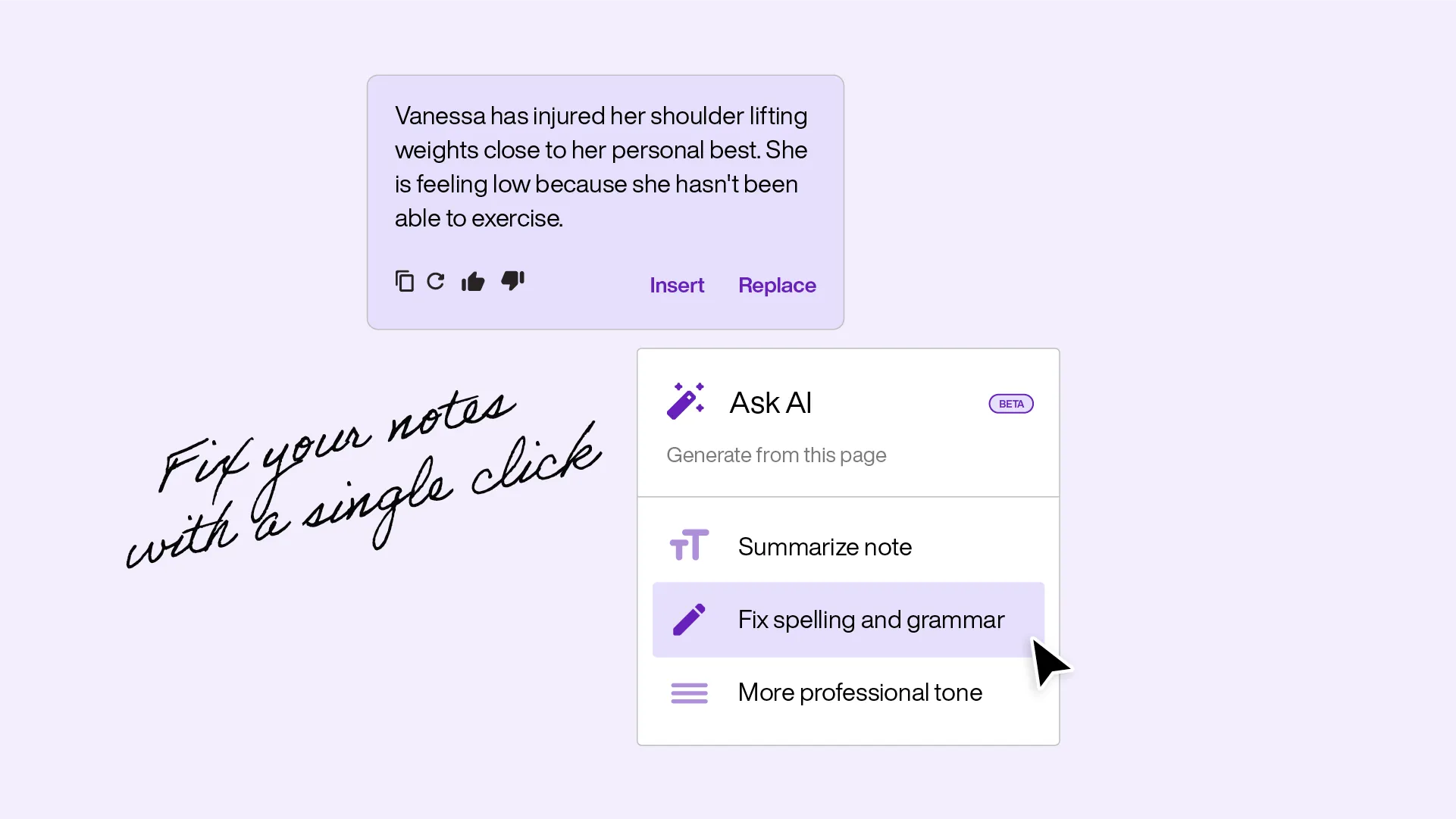
AI transcribe
Quick notes, fixed
AI summarises notes in a click. Your clinical documentation reads the way it should, without you spending the time to polish it.
- Highlight any text and summarise with one click
- Grammar, spelling, and punctuation cleaned automatically
- Insert alongside or replace the original text
Trusted
Secure and compliant
HIPAA and GDPR compliant. Encrypted storage with full audit trails. Your documentation meets the standard without you having to think about it.
- Electronic provider signatures for sign-off
- Note locking to authorised practitioners on finalised records
- Encrypted storage with HIPAA and GDPR compliant audit trails