


What is a physical examination?
A physical examination is a crucial component of patient assessment and medical care. It involves a healthcare provider systematically evaluating a patient's body systems to gather objective data about their health status and the patient's health status. A physical exam aims to identify any signs of disease, injury, or abnormality that may require further investigation or treatment (Garibaldi & Elder, 2021).
The healthcare provider uses various techniques to assess the patient's overall health and specific body systems during a physical examination. This information also helps inform the patient's treatment plan.
Different parts of a physical exam
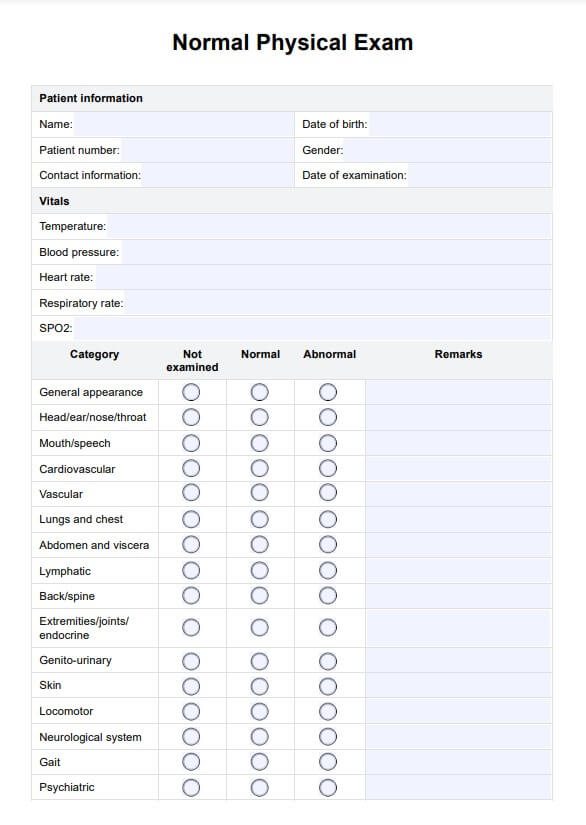
A physical exam is a comprehensive assessment of a patient's health. Here's a breakdown of the critical components:
- Vital signs: Blood pressure, heart rate, respiratory rate, and temperature provide a baseline health assessment.
- Physical appearance and mental status: This includes observing mood, affect, and communication ability.
- Skin, hair, and nails: Examined for color, texture, moisture, and abnormalities like rashes or lesions.
- Head, eyes, ears, nose, and throat (HEENT): Checks head for trauma, visual acuity, ears, nose, throat, and oral health.
- Neck and lymph nodes: Palpated for tenderness, stiffness, or enlarged lymph nodes. The thyroid gland is also assessed.
- Chest and lungs: The chest wall is inspected for symmetry and signs of deformity. Lungs are auscultated for breath sounds.
- Cardiovascular system: Pulses are checked for rate, rhythm, and quality, and the heart is listened to for abnormal sounds.
- Abdomen: Inspected for contour, symmetry, and masses. Bowel sounds are auscultated, and the abdomen is palpated for tenderness or masses. The liver and spleen are assessed.
- Musculoskeletal system: The upper and lower extremities' muscle strength, normal gait, tone, and symmetry are evaluated. The range of motion of major joints is assessed for limitations, pain, or crepitus. The spine is inspected for abnormalities. Gait and ability to perform daily activities are observed.
- Neurological exam: Cranial nerves, motor function, sensory function, and reflexes are tested. Coordination, balance, and fine motor skills are assessed for abnormalities.









