What is a Nurse Assessment Sheet Template?
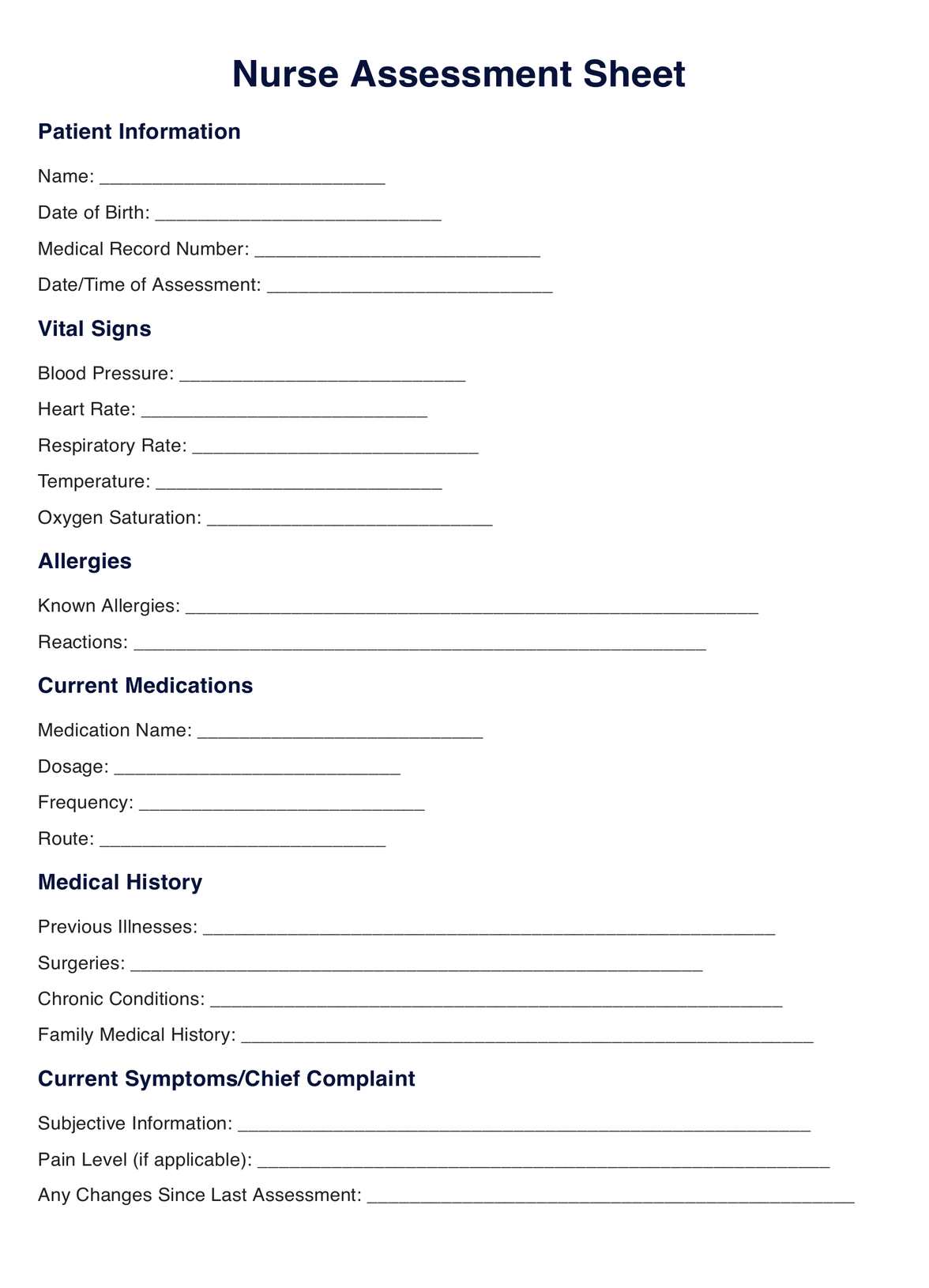
A Nurse Assessment Sheet Template is a structured document designed to assist healthcare professionals, particularly nurses, in systematically gathering and recording essential information about a patient's health status.
This tool serves as a framework for conducting comprehensive assessments and ensures that all relevant aspects of a patient's condition are thoroughly evaluated.
The template typically includes sections covering a patient's health facets, such as vital signs, medical history, current symptoms, allergies, medications, and existing chronic conditions.
It provides a standardized format to document subjective and objective data obtained during the assessment process, promoting consistency and clarity in healthcare records.
The vital signs section of the template may include fields for recording measurements such as blood pressure, heart rate, respiratory rate, and temperature.
Another section may focus on the patient's medical history, prompting the nurse to document information about previous illnesses, surgeries, and family medical history.
Furthermore, the template often incorporates space for nurses to record their observations and assessments of the patient's physical appearance, cognitive function, and emotional well-being. This holistic approach enables healthcare professionals to consider the immediate health concerns and the broader context of the patient's overall well-being.
Using a template enhances communication among healthcare team members and contributes to continuity of care. It also aids in tracking changes in a patient's condition over time, facilitating better-informed decision-making.
Additionally, these templates are valuable for documentation purposes, meeting regulatory requirements, and supporting quality improvement initiatives within healthcare settings.









